
Patient safety culture and handoff evaluation of nurses in small and medium-sized hospitals
2021-02-28 09:48JungHeeKimJungLimLeeEunMnKim
Jung Hee Kim ,Jung Lim Lee ,Eun Mn Kim
a Department of Nursing Science,Shinsung University,Chungnam,South Korea
b Department of Nursing,Daejeon University,Daejeon,South Korea
c Department of Nursing Science,Sun Moon University,Chungnam,South Korea
Keywords:Evaluation studies Handoff Hospital nursing staff Patient safety
ABSTRACT Objectives:This study was conducted to investigate the current status of handoffs,perception of patient safety culture,and degrees of handoff evaluation in small and medium-sized hospitals and identified factors that make a difference in handoff evaluation.Methods:This is a descriptive study.425 nurses who work at small and medium-sized hospitals in South Korea were included in our study.They completed a set of self-reporting questionnaires that evaluated demographic data,handoff-related characteristics,perception of patient safety culture,and handoff evaluation.Results:Results showed that the overall score of awareness of a patient safety culture was 3.65 ± 0.45,the level was moderate.The score of handoff evaluation was 5.24±0.85.Most nurses experienced errors in handoff and most nurses had no guidelines and checklist in the ward.Handoff evaluation differed significantly according to the level of education,work patterns,duration of hospital employment,handoff method,degree of satisfaction with the current handoff method,errors occurring at the time of handoff,handoff guidelines,and appropriateness of handoff education time (P < 0.05).Conclusion:For handoff improvement,guidelines and standards should be established.It is necessary to develop a structured handoff education system.And formal handoff education should be implemented to spread knowledge uniformly.
What is known?
·Small and medium-sized hospitals have become a patient safety blind spot although they play a crucial role.
·Handoff is recognized as an important aspect of patient care to ensure the safety and continuity of care to optimize patient outcomes.
What is new?
·For handoff improvement,guidelines and standards should be established and processes should be modified.
·It is necessary to develop a structured handoff education system.And formal handoff education should be implemented to spread knowledge uniformly
1.Introduction
Small and medium-sized hospitals play a key role in South Korea’s medical services as secondary health care centers and comprise 93.8% of all hospitals in the nation [1].Small and medium-sized hospitals also carry out the central task of providing easy access to hospitals and health care services for local residents[2].However,these hospitals may not be as competitive as large hospitals in service quality and patient safety.An adequate supply of qualified nurses is an essential factor for improving care quality.However,ensuring a sufficient nursing workforce in small and medium-sized hospitals can be a challenge for them,due to excessive work hours,low wages,and poor work environments.
The nursing shortage in small and medium-sized hospitals is a systemic issue that tends to increase the occurrence of errors and related adverse incidents during the performance of nursing tasks[3].Small and medium-sized hospitals have become a patient safety blind spot although they play a crucial role in the national health-care-delivery system.Factors that contribute to this problem include insufficient opportunities for education,communication issues,nurses’ inattention to improving the quality of work,and system inadequacy and workforce insufficiency for facilitating quality improvement in addition to nursing shortages [4].As a consequence,job satisfaction is low,reducing enthusiasm for participation in activities to improve patient safety[5].Also,nurses in small and medium-sized hospitals are severely isolated because nursing education and efforts for work improvement almost exclusively occur in large university hospitals in metropolitan areas that have established systems and a larger workforce.
Handoff is defined as the exchange of information,responsibility,and accountability between nurses about patients at shift change[6,7].Handoff is recognized as an important aspect of patient care to ensure the safety and continuity of care to optimize patient outcomes.Ineffective handoffs have been estimated to be responsible for about 40% of adverse events,such as treatment errors and patient death [8]; moreover,around 22% of adverse events associated with nursing care align with poor communication during handoffs [9].Therefore,from the clinical practice perspective,several international institutions have recognized nursing handoffs as a priority area for improvement[10,11].
What makes a handoff ineffective is supplying incomplete or erroneous information to the incoming nurse,inefficient methods of communication,and insufficient duration for handoffs,interruptions or disruption of handoffs,absence of standardization of handoff methods,and workforce shortages [12].As handoffs are increasingly being recognized as an essential element of patient safety in the United States,Australia,and Europe,stakeholders are making various attempts to standardize primary content and templates for handoffs,developing handoff tools or methods,improving the quality of handoffs,providing an opportunity to ask questions during handoffs,education or training about handoffs,and conducting bedside handoffs [13,14].
Monitoring the quality of nursing handoff is an important responsibility of the hospital toward its patients for quality improvement and patient safety[15].And efforts should be made to identify and improve the factors affecting efficient handoff.Richter,McAlearney,and Pennell [16]proposed the conceptual framework to explain the relationships between the perception of patient handoffs and organizational factors on patient safety.They suggested that conducting a safety culture has enabling,enacting,and elaborating phases that influence patient safety and handoff.Strong teamwork culture and management support culture was found to enhance effective handoff of patient information and responsibility of all occupations of the hospital[17,18].Handoff error experience,the frequency of events reported,and the presence of standardized guidelines were the factors to the handoff evaluation of nurses[17,19].While these studies were conducted on the relationship between patient safety culture and handoff,they were not focused on the handoff by nurses or were conducted with nurses in special parts,such as delivery rooms and newborn units.
Moreover,previous studies about handoffs in South Korea have focused on large hospitals and did not consider small and mediumsized hospitals,where the structure of the workforce and the nursing care delivery system are different [19-22].
Therefore we investigated the current status of handoffs,perception of patient safety culture,and degrees of handoff evaluation in small and medium-sized hospitals and identified the factors that make a difference in handoff evaluation.We aimed to provide foundational data that can be considered while developing interventions that can help improve nursing handoffs in small and medium-sized hospitals that are weak in the areas of professional education or work modification.
2.Participants and methods
2.1.Study design
This is a descriptive study investigating the current status of handoffs,perception of patient safety culture,degrees of handoff evaluation,and identifying the factors that make a difference in handoff evaluation in small and medium-sized hospitals.
2.2.Participants
We performed a convenience sampling of nurses working in small and medium-sized hospitals that had 150 to 400 beds.Inclusion criteria included nurses who (a) were nurses on duty,(b)had at least six months of working experience,and(c)understood the aims of our study.Exclusion criteria included nurses who (a)were nurses in training,(b) had no experience in the handoff.We used the G-power 3.1.3 to determine the sample size.Calculation results with 0.15 assigned to effect size,0.95 to the significance level,and 10 to the number of predictors in our linear regression analysis suggested that we needed 172 participants.We distributed surveys to 435 nurses in eight hospitals and retrieved answers from 430 respondents.Excluding responses that were poorly completed,we analyzed data from the remaining 425 respondents.
2.3.Measures
2.3.1.General characteristics
General characteristics consisted of the participant’s age,sex,level of education,work department,work patterns,and work experience.
2.3.2.Handoff-related characteristics
The handoff-related characteristics consisted of 10 items.Kim et al.[22]developed 7 items,which were handoff methods,satisfaction with the current handoff method,reasons for dissatisfaction with the current handoff method,error when handing over,error when taking over,presence of handoff guidelines,and appropriate methods for improving the handoff.The authors of this study added three handoff-related education items,which were timing of handoff education,handoff education method,and appropriateness of handoff education time.As handoff-related characteristics are nominal-scale measurements,each item obtains the percentile of categories.
2.3.3.Perceptions of a patient-safety culture
To evaluate nurses’perceptions of the patient safety culture,we used the Patient Safety Survey Questionnaire,which is a Korean version translated by Kim et al.[23]of the Hospital Survey of Patient Safety Culture,developed by the Agency for Healthcare Research and Quality in the United States [24].The 37 questions were measured on a 5-point Likert scale.A high score suggests a positive perception of patient safety.The evaluation survey for patient safety consisted of five subdomains:overall evaluation of patient safety (1 item); manager’s awareness of patient safety (5 items); reasonable communication and processes (13 items); the degree of cooperation among departments and units (14 items);and frequency of medical errors reported (4 items).We measured the reliability of this instrument using Cronbach’s α values,which were 0.73 for the manager’s awareness of patient safety,0.90 for interdisciplinary collaboration in the hospital,0.87 for communication and procedures,and 0.90 for the frequency of reported medical errors.
2.3.4.Handoff evaluation
In this study,we used a modified version of the handoff evaluation instrument by Kim et al.[20]that appeared in O’Connell et al.[15]after translating it into Korean.The 18 questions were measured on a 7-point Likert scale.The handoff evaluation survey consisted of five subdomains:quality of information(5 items);the degree of interaction and support during handoff (3 items); efficient time and information delivery (2 items); sufficient patient information (4 items); and structure,procedure,and quality of handoff (4 items).A higher score means a better evaluation,and reliability in this study was Cronbach’s α=0.95.
2.4.Data collection
This study received IRB approval from the College of Nursing at Sun Moon University(IRB number SM-201911-072-1)to ensure the ethical protection of the research participants.First,we obtained permission from nursing directors at the affiliated medical institutes and explained our research goal and study methods to participants before conducting the survey and site investigation.Finally,we received written informed consent and conducted the survey,after assuring the participants that the data retrieved will be treated anonymously.
2.5.Data analysis
We performed an analysis of the collected data using the SPSS/WIN 22.0 program.The details of the analysis follow:1)We analyzed the general characteristics of respondents and their handoff-related characteristics using descriptive statistics such as frequency,percentile,mean,and standard deviation; 2)we analyzed participants’;evaluation of handoffs and perceptions of a patient-safety culture using descriptive statistics such as the mean and standard deviation; 3)we analyzed differences in the evaluation of handoffs by general characteristics and handoff-related characteristics using the independent t-test and ANOVA and the Scheff′e post hoc test.
3.Results
3.1.General characteristics of participants
The general characteristics of the participants appear in Table 1.The mean age of participants was 31.6 ± 8.33 years and the mean duration of hospital employment was 78.36 ± 75.77 months.
3.2.Handoff-related characteristics
Characteristics related to handoffs appear in Table 2.When asked if they were satisfied with the current method of handoffs,245 respondents(57.6%)answered satisfied.Regarding reasons for dissatisfaction,the handoff interruption (31.4%) was ranked highest.Of all study participants,only 21 (5.0%) answered that there was no error when they engaged in handoffs,whereas 48 (11.3%)answered there was no error when they received handoffs.A total of 329 respondents(77.4%)responded that they had no guidelines or checklists about handoffs for the hospital ward.
Regarding the timing of handoff education,“after being placed in ward” was the highest with 386 participants (76.7%).Regarding how handoff education was performed,241 participants (45.6%)and 239 participants(45.2%)answered it was done mostly by peer nurses’ oral teachings and their observations,respectively.When asked about the duration of handoff education,250 participants(58.8%) answered that handoff education time is insufficient.Regarding methods for handoff improvement,218 participants(27.7%) thought that there is a need for hospital-wide handoff education or on the departmental level.
3.3.Perception of a patient safety culture and handoff evaluation
Participants’ perceptions of patient safety culture and average handoff evaluations appear in Table 3.The overall score of awareness of a patient safety culture was 3.65 ± 0.45.The score of the handoff evaluation was 5.24 ±0.85.
3.4.Differences in handoff evaluations for general and handoffrelated characteristics
The difference in handoff evaluations for general and handoffrelated characteristics appear in Table 4.Nurses who graduated from the 4-year program have higher handoff evaluation than those with other education levels (P=0.013).There is a difference in handoff evaluations among nurses who have different work patterns(P=0.010).Nurses with 12 months working life have higher handoff evaluation than those with a working life of 37-84 months(P=0.004).Nurses who use verbal handoffs using Kardex or verbal handoffs referring to EMR have higher handoff evaluation than those who use other methods (P=0.004).Nurses who were satisfied with the current handoff method have higher handoff evaluation than those who didn’t (P < 0.001).Nurses who didn’t experience an error when handing over have higher handoff evaluation than those who experience error (P=0.002).Nurses who didn’t experience an error when taking over have higher handoff evaluation than those who experience error (P < 0.001).Nurses who had both handoff guidelines and checklist have the highest handoff evaluation and nurses who had no guideline and no checklist have the lowest handoff evaluation (P=0.005).Nurses who thought handoff education time was appropriate have higher handoff evaluation than those who didn’t (P <0.001).
4.Discussion
Handoffs between nurses is a form of essential communication taking place in hospitals,and significantly affects patient safety and medical-service quality.We conducted this study to provide an overview of the current status of handoffs and to identify factors that make a difference in handoff evaluation in small and mediumsized hospitals.
Handoff evaluation is a multilateral evaluation of handoffs in use.The level of handoff evaluation for participants in this study was moderate.Of all subdomains,the quality of information was highest,and the structure,process,and quality of handoffs were lowest.This is higher than the score of emergency room nurses[20]but is lower than that of delivery rooms/newborn nursery nurses[19],indicating a need for improvement in handoffs.When a written guideline is available and when sufficient education is provided,the handoff evaluation was significantly higher.Therefore,to improve clinical handoff,the related standard and guidelines should be established in advance,and education about them should be provided sufficiently [23].This process can improve the structure,process,and quality management of handoffs.
The level of patient safety culture perception for participants inthis study was moderate.Of all subdomains,managers’ awareness of patient safety was the highest,and the degree of cooperation among departments and units was lowest.This result is in line with previous research results[19,20].Nursing handoffs can be classified into intradepartmental or interdepartmental handoffs.Intradepartmental,as well as interdepartmental team efforts,promotecollaboration and communication to accommodate an effective handoff of patient information and can improve patient safety[17-20].Therefore,individual efforts and various hospital-wide endeavors should be created to promote team efforts in establishing interdepartmental collaboration systems.As cooperation among departments and units is the important factor of handoff evaluation in previous studies [19,20],efforts should be made to promote cooperative relations between departments.
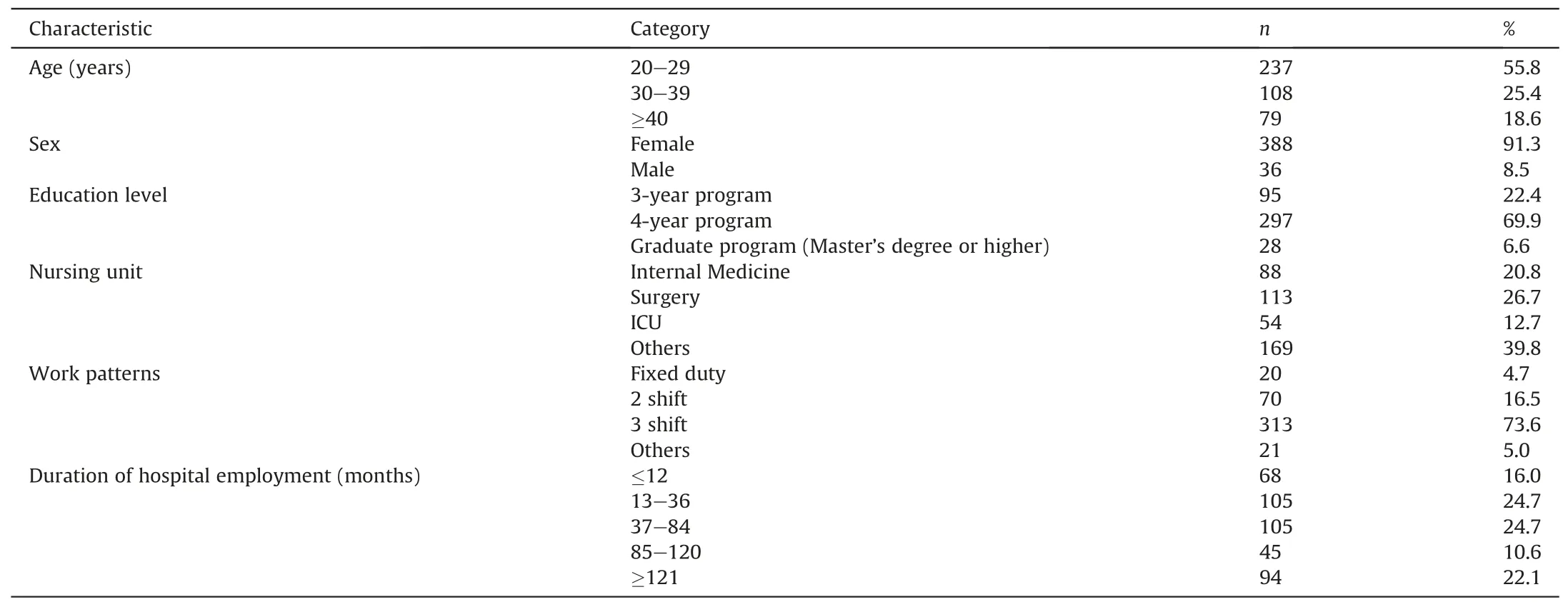
Table 1 General characteristics of the participants (N=425).
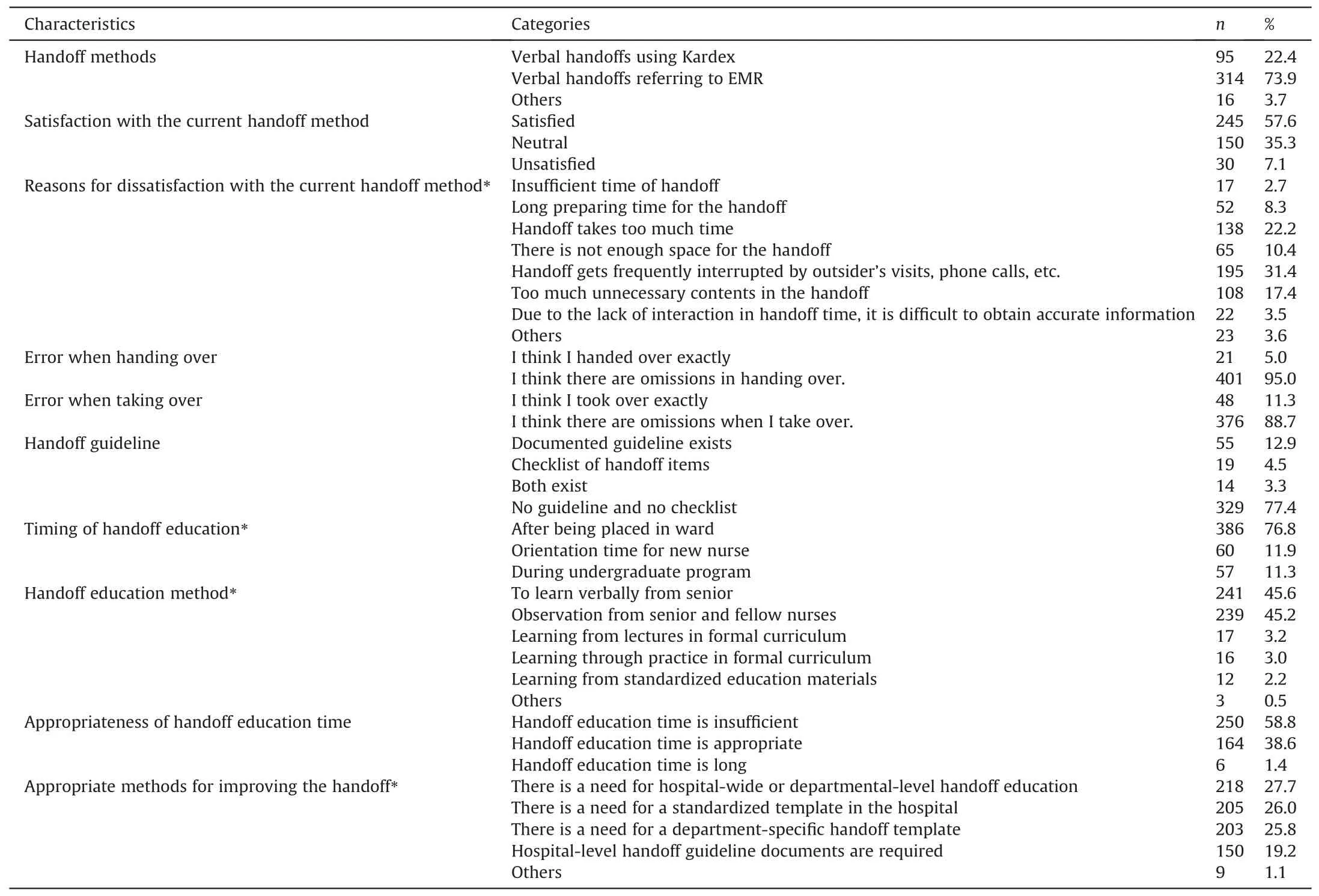
Table 2 Handoff-related characteristics (N=425).

Table 3 Perception of patient safety culture and handoff evaluation.
Factors significantly making a difference in handoff evaluation by nurses in small and medium-sized hospitals were level of education,work patterns,duration of hospital employment,handoff method,degree of satisfaction with the current handoff method,errors occurring at the time of giving the handoff,errors occurring at the time of receiving the handoff,handoff guidelines,and appropriateness of handoff education time.This finding is consistent with results from previous studies showing a significant relationship among the handoff method,degree of satisfaction with the handoff method,errors occurring at the handoff time,and handoff evaluations [17-22].
We found 57.6% of nurses were satisfied with the current method of handoffs.Regarding currently used handoff methods,the level of satisfaction was lower for nurses in small and mediumsized hospitals than among those in emergency rooms(67.3%)[20]and delivery rooms/newborn nurseries (75.3%) [19].Because satisfaction with the current handoff method is also a significant factor to handoff,it is necessary to conduct an in-depth exploration of the reasons for dissatisfaction with handoff methods.Besides,considering the results from a previous study[20]and the present study,the handoff via electronic medical record(EMR)is increasing regardless of the hospital size.Therefore,the experiences and opinions of the nurses about the EMR-based handoff method should be investigated and positively reflected in the development of an EMR-based handoff program and the establishment of a handoff process.
The appropriateness of handoff education time and the error when taking over were also found to be the factors to the handoff evaluation by the experience in handoff errors identified in a previous study[19].The previous study also showed that the absence of guidelines and checklists and an inadequate handoff system as the cause of handoff errors are also factors to the handoff evaluation [19].
In this study,only 8.4%of all respondents said that they received handoff education as part of an official course in the form of lectures,training sessions,and standardized education materials.In comparison,90% of them acquired the necessary skills through verbal teachings from senior nurses or through observations.Also,77.4% of small and medium-sized hospitals had no written guidelines or checklists about handoffs.Previous studies in South Korea revealed 51.5%-57.6% with more than 500 beds [19]also had no written guidelines or checklists.Considering that 64% of British institutions[25]had no written guidelines or checklists either,our results revealed the higher vulnerability of small and mediumsized hospitals in South Korea.
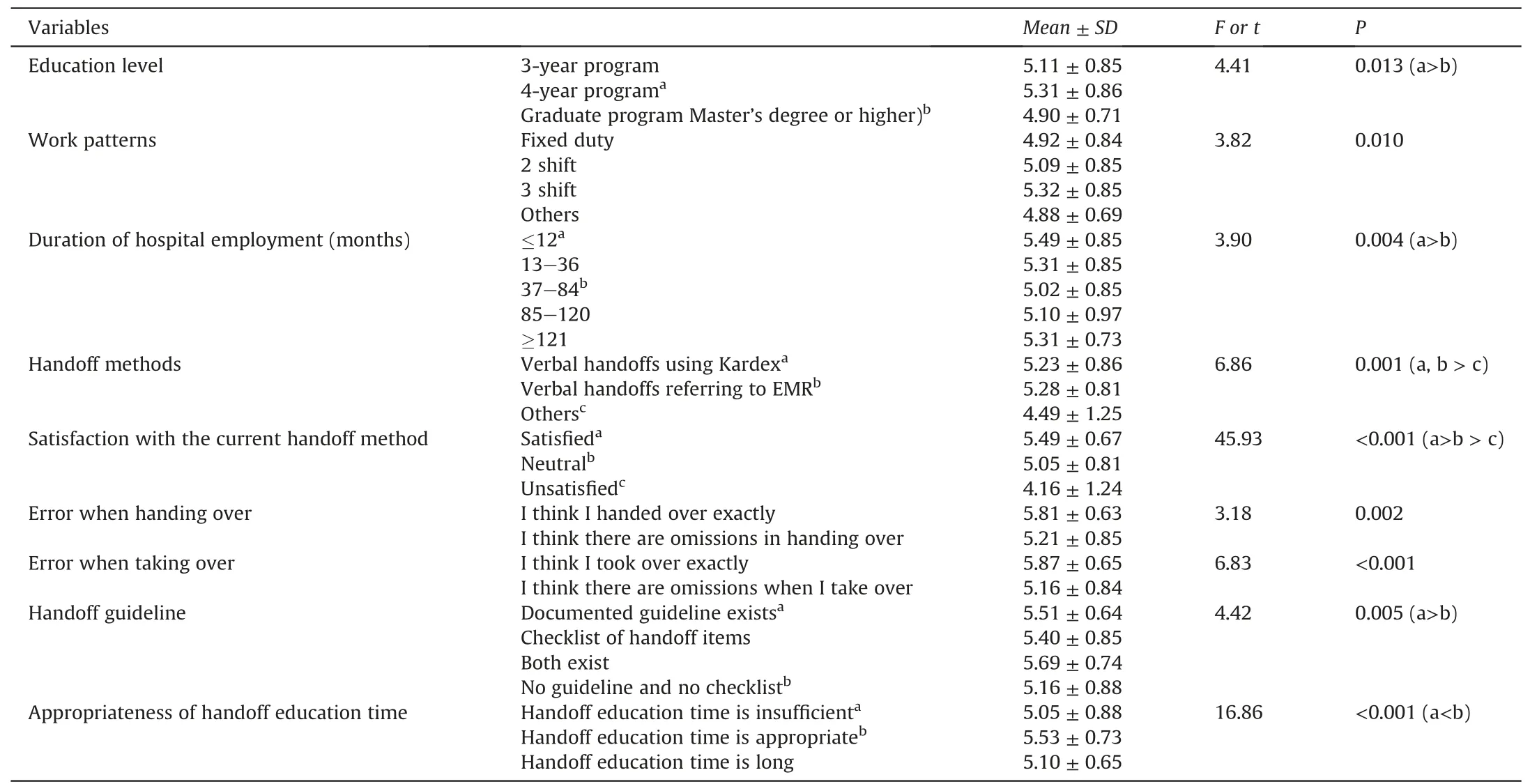
Table 4 Differences in handoff evaluation by demographic data and handoff characteristics.
Organization guidelines and standards should exist for a standardized handoff system,and formal education should be implemented [26].Therefore,for handoff improvement in small and medium-sized hospitals,the establishment of relevant guidelines and standards should precede official education activities such as new nurse orientation or on-the-job training.
In the healthcare accreditation of Korean and overseas medical institutions,whether a standardized communication tool is used for patient safety is considered in the evaluation,wherein one of the representative forms of communication is handoff[6,10,11].The establishment of a handoff system starts by designing organizational guidelines and standards.Besides,handoff standardization can be acquired by implementing various methods of handoff improvement that correspond to the characteristics of institutes as well as of users.For accurate and efficient handoff,tools such as SBAR (situation,background,assessment,recommendation) are used to standardize the details of handoff and prepared them as a template to be consistently used by the staff[6,14].Besides,bedside handoff can increase patient satisfaction by encouraging patient and family involvement and reduce handoff errors and patient safety accidents [13].
Standardized handoff methods should be transmitted to the nurses through formal education.Finally,handoff quality and the outcomes of handoffs should be monitored periodically and continuously.
5.Limitation
The present study has the limitations described below and thus requires caution in the interpretation of the results.We herein suggest further studies to overcome the limitations and contribute more to the improvement of handoff at clinical sites.Firstly,since the subjects of this study were small and medium-sized hospitals,the effect of the hospital size on the results was not investigated.Since the systems or the scope of available resources may depend on the size of the hospital,we suggest replication studies with hospitals of different sizes to acquire the results that reflect the characteristics of medical institutions.Second,the subjects of the present study include those who use written Kardex for handoff and those who use EMR for handoff.Hence,the effect of the handoff method on the handoff evaluation was not investigated.In particular,the propagation of EMR,which has a huge advantage in the acquisition and organization of information,has a significant effect on the handoff.Therefore,we propose further studies on the handoff evaluation and the handoff promotion strategy,focusing on the handoff via EMR.These studies are well-matched with the demand for clinical sites and will make an important contribution to patient safety.Finally,we suggest an in-depth exploratory study on the handoff-promoting factors and handoff-inhibiting factors to establish an accurate and efficient handoff method.
6.Conclusion
This study provides essential data for developing an intervention that can help improve nursing handoffs by investigating handoff characteristics,handoff evaluations,and patient safety culture perception of nurses working in small and medium-sized hospitals and identifying factors making a difference in the handoff evaluation.
Study results showed that factors making a difference in handoff evaluation by nurses in small and medium-sized hospitals were level of education,work patterns,duration of hospital employment,handoff method,degree of satisfaction with the current handoff method,errors occurring at the time of giving the handoff,errors occurring at the time of receiving the handoff,handoff guidelines,and appropriateness of handoff education time.For handoff improvement,guidelines and standards should be established,based on our findings,and processes should be modified.It is necessary to develop a structured handoff education system.And formal handoff education should be implemented to spread knowledge uniformly.Based on study findings,we recommend future studies focus on the development of standardized handoff methods suitable for small and medium-sized hospitals and on an evaluation of their effect on patient safety and nursing quality following their implementation.
Funding
This research was supported by the National Research Foundation of Korea (NRF-2019R1I1A3A01059093)
CRediT authorship contribution statement
Jung Hee Kim:Conceptualization,Methodology,Investigation,Resources.Jung Lim Lee:Data curation,Formal analysis,Writingoriginal draft.Eun Man Kim:Conceptualization,Methodology,Investigation,Formal analysis,Writing-original draft.
Declaration of competing interest
The authors declare no conflict of interest.
Appendix A.Supplementary data
Supplementary data related to this article can be found at https://doi.org/10.1016/j.ijnss.2020.12.007.
 International Journal of Nursing Sciences2021年1期
International Journal of Nursing Sciences2021年1期
- International Journal of Nursing Sciences的其它文章
- Focuses and trends of the studies on pediatric palliative care:A bibliometric analysis from 2004 to 2018
- Relationship between negative emotions and perceived support among parents of hospitalized,critically ill children
- The effect of digital health technologies on managing symptoms across pediatric cancer continuum:A systematic review
- Effectiveness of animal-assisted therapy on pain in children:A systematic review and meta-analysis
- Effects of creative expression program on the event-related potential and task reaction time of elderly with mild cognitive impairment
- Struggling to live a new normal life among Chinese women after losing an only child:A qualitative study