
Impact of resistance exercise training on physical performance of patients undergoing hemodialysis
2022-12-19 02:21AhmedLateefAlkhaqani
TMR Non-Drug Therapy 2022年4期
Ahmed Lateef Alkhaqani
1Ministry of Health,Al-Najaf Direction,Al-Sadder Medical Hospital,Al-Najaf 00964,Iraq.
Abstract
Keywords:resistance exercise;physical performance;hemodialysis
Background
Chronic kidney disease (CKD) is a general medical problem worldwide. It is one of the most common causes of disease and death worldwide, especially in developing countries, as a global public health problem [1]. In addition, the prevalence of end-stage kidney disease (ESKD) renal replacement therapy (RRT) has increased dramatically since the 1960s. International comparison of chronic kidney disease prevalence is challenging due to the different methods for the assessment of kidney dysfunction, such as decreased estimated GFR (eGFR), proteinuria, hematuria, uncontrolled hypertension, pain,e.g., loin pain, burning on micturition, dyspnea on exertion,peripheral oedema (pitting oedema to extremities) and the use of different definitions of CKD[2].
According to the reported “World Health Organization”, “physical inactivity is already a major global health risk and prevalent in both industrialized and developing countries, causing approximately 5.2 million deaths.Physical inactivity is the primary cause of most chronic diseases, and it is one of four main risk factors of CKD”. In today’s world, physical activity is very important. Exercise keeps the body strong and healthy [3]. Therefore, increased physical activity is essential to preventing and managing chronic kidney disease [4]. The National Institute for Health and Care Excellence (NICE) in guidelines on chronic kidney disease in adults, recommends: encouraging people with CKD to take exercise, achieve a healthy weight, and stop smoking. The American National Kidney Foundation (ANKF)guidelines include a similar statement encouraging exercise, weight loss, and smoking cessation in CKD. Physical activity promotes a variety of metabolic benefits that can reduce the long-term risk of progression of kidney dysfunction[5].As patients with chronic kidney disease are prone to muscle loss and weakness, physical function preservation is of particular importance and appropriate exercise,therefore, has the potential for reduced morbidity and associated cost savings [6]. Patients undergoing hemodialysis suffer from deteriorating physical health, impaired physical function, and have a low quality of life, that explained by insufficient metabolic clearance.To overcome these obstacles, cost-effective strategies must be developed, including exercise as a complement to hemodialysis therapy.
Study significance
Global burdens of CKD are rising, and by 2040 it is expected to become the world’s fifth most common cause of death. The problem can prevent patients from carrying out daily activities.As a result,low physical performance is the most common complication of chronic kidney disease, and low physical activity and disability are associated with a greater risk of disability and death. In addition, patients with CKD on maintenance hemodialysis (HD) suffer from a progressive deterioration of impaired physical function, which is associated with increased mortality and morbidity and decreased quality of life and leads to decreased physical activity of patients[7].Patients’quality of life undergoing hemodialysis can be affected by social factors causing major changes in the life of patients with CKD,also affected by clinical changes caused by the disease and its complications. Information on this subject can therefore help to identify risky patients. The decrease in hemolysis patients’ life expectancy can affect various aspects of their lives. Impaired quality of life can change the patient’s functional status from the physical perspective. So that the patients’ daily physical activity is disrupted, and their ability to perform daily activities is decreased. Changes in lifestyles and their limitations have influenced and impacted patients and their families, ultimately reducing their quality of life.
Despite this, exercise programs are not commonly implemented in dialytic routines in many countries due to many existing barriers that healthcare professionals have to face when proposing an exercise intervention during dialysis.These barriers include lack of knowledge,fear of injury or medical complications, fatigue, or simply a lack of motivation by the patient and the healthcare professional. Many studies focus on overcoming these barriers. For example, nurse-led exercise interventions have been proven efficient in physically impaired populations, such as the elderly, complex ambulatory, or diabetic patients. In studies involving CKD patients, these interventions have also improved clinical outcomes and reduced hospitalization rates. Although it is increasingly recognized that physical activity needs to be promoted, the existing evidence base for the cost-effectiveness of relevant interventions appears to be weak and dispersed. This experimental study will contribute to the important topic in medical studies to fill and address the literature gap. This study aimed to evaluate the physical performance of patients undergoing hemodialysis by a short physical performance battery(SPPB) scale and to determine the effectiveness of exercise training in improving the physical performance of hemodialysis patients.
Resistance exercise training as a rehabilitation
Resistance training (also referred to as strength training or weight training) progressive uses different loads, movements, and speeds to improve muscles’ strength, strength, and resistance. Resistance exercise is one of the modalities of exercise chosen for physical conditioning. The process of post-injury rehabilitation is shifting from preventive prevention by resistance training to preventive prevention of injury [8]. The American Diabetes Association, 2014 reported that lifestyle modifications(such as diet and exercise)were associated with a greater decrease in blood sugar control compared to medication emphasizing aerobic exercise training[9].Evidence:There are various guidelines (mainly the American Heart Association and the American College of Sport and Medicine) for describing resistance exercise training in healthy populations and populations with different co-morbidities and different age groups [10]. Evidence suggests that resistance training is more important in improving functional mobility than aerobic training for older adults [9].
Study hypothesis
Patients who attend resistance exercise programs exhibit better physical performance than before.
Methods
Study design
The experimental design (Randomized Controlled Trial) will be implemented in the study by which the patients will assign randomly into two groups (study and control groups).
The study’s setting will take place in Al-Najaf Al-Ashraf City/Al-Najaf Health Directorate/Al-Sadder Medical City/Hemodialysis Center and Al-Hakeem General Hospital/Al-Hakeem Hemodialysis Center.
Ethical considerations
All the participants signed informed consent form. The study was approved by the University of Kufa/College of Medicine-Medical Ethical Committee(ethical number: 19).
Study population
All the patients are undergoing hemodialysis in Al-Najaf city.
Participants selection
According to the American Society of Nephrology clinical practice guidelines for chronic kidney disease diagnosis [11], 68 patients volunteers eligible will be recruited participate the study who was admitted there during the study period (34 participants will be selected purposively from each centre, Al-Hakeem General Hospital,and Al-Sadder Medical City/Hemodialysis Center). Patients with chronic renal disease who are admitted to hemodialysis meet the eligibility criteria for participation.
Randomization (groups assignment)
63 patient samples will be randomly divided into two groups. The study group consists of 32 patients who the researcher will expose to resistance exercise training programs. The group that didn't expose to the resistance exercise training program by the researcher is the control group, consisting of 31 patients.
After the initial assessment, the randomly assigned patient is executed using a random number list generated by the computer via(an Excel table) researcher is prepared to eliminate bias in intervention tasks. The study adheres to the procedures for maintaining the separation of the study and the control group. To avoid contact, patients were assigned to each group every week. See Figure 1.
Blinding
The researcher uses the double-blinded technique in the present study,and it’s used between the investigator and the patients for the data collection outcomes.Therefore, the participants and researcher do not know the study group and the control group. In addition, both the study and the control group were treated equally after it was randomly assigned (administering the data collection instruments and ethical protocol except for the intervention).
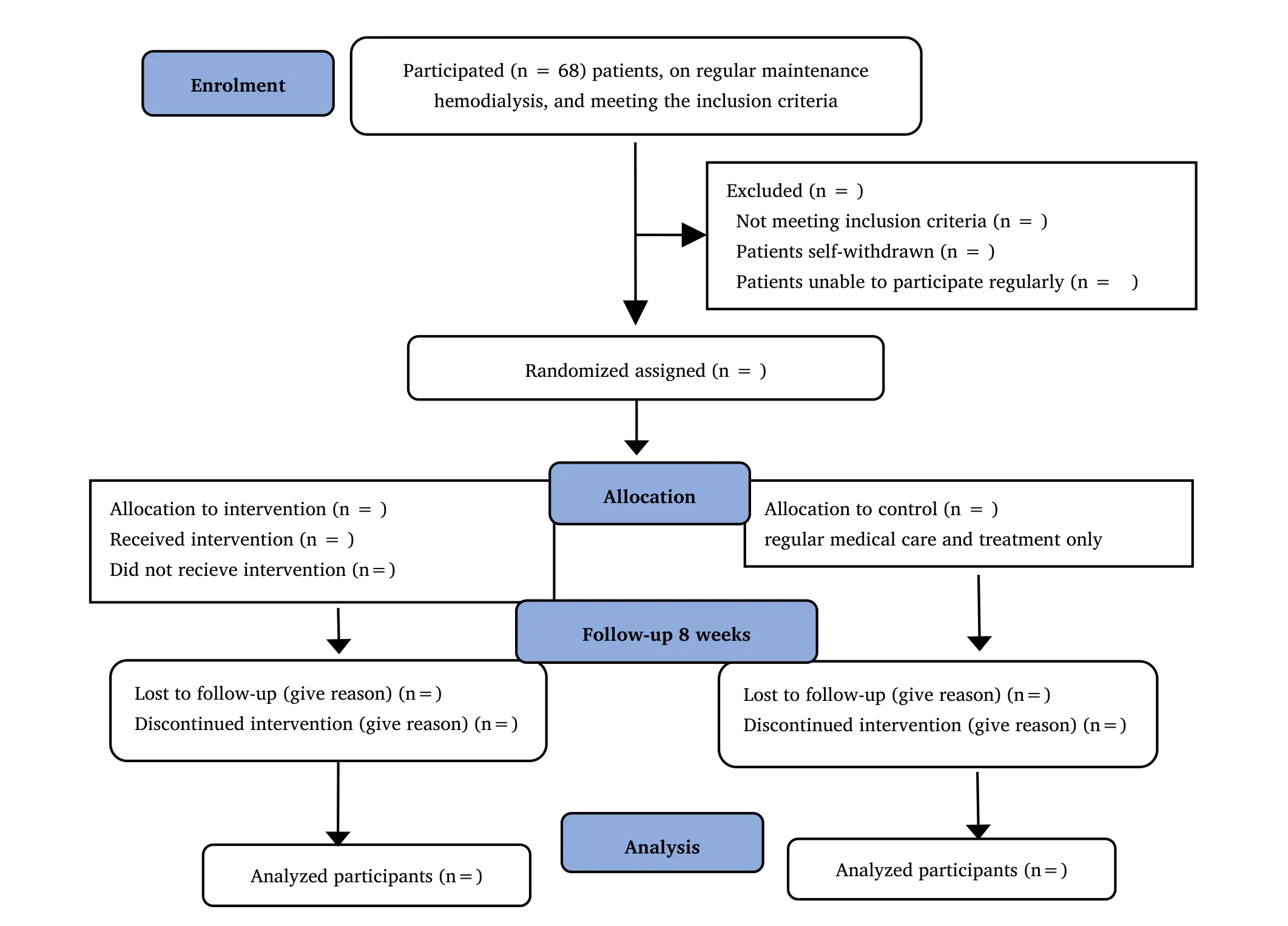
Figure 1 Participant’s flowchart
Sample of the study
A non-probability(purposive sample)technique selected from patients undergoing hemodialysis will be included in the present study. All patients who visit the Al-Hakeem General Hospital and Al-Sadder Medical City/Hemodialysis Center on hemodialysis are medically diagnosed with chronic kidney disease and undergoing hemodialysis.The sample will be assigned randomly into study and control groups.This study sample will be selected based on the following criteria:
· All participants receive more than two sessions a week because rehabilitation programs cannot be used for patients receiving less than two sessions a week. In addition, it lacks to show progress in physical performance due to the time spacing between sessions, that be according to policy and rules of the Oklahoma Health Care Authority (OHCA).
· The participants are between 20 years and older; the present study focused on adult patients, and CKD most commonly occurs in adult patients compared to young patients.
· All participants are from Iraqi Nationality to facilitate the communication.
· Alert patients and free from changes in consciousness level because studies require subjective measurement.
· Patients who are free from psychiatric disorders because the researcher needs to explain and clarify the steps of participation in the program; it depends on the patient’s cooperation.
· Participants who are undergoing hemodialysis for at least six months; and are medically stable; in order to avoid complications.
· Patients are able to carry out the exercise.
Exclusion criteria
Patients with kidney disease in the final stages of a relative or absolute contraindication to exercise tests. These conditions include:
· Lower-extremity fracture or amputation.
· Patients with limitations in walking ability.
· Mechanical disorders associated with pain (such as lumbar disk or lumbar spondylosis).
· Cerebral vascular diseases manifested as transient ischemic attacks.
· Chronic lung diseases result in significant oxygen desaturation during exercise or pulmonary congestion; the program’s application requires patients’ compliance and may cause fatigue.
· Cardiovascular diseases such as angina at rest or on exertion.
· To avoid vascular access failure and complication,patients with vascular access in a lower extremity(femoral catheter).
Inclusion and exclusion criteria are listed based on methodological and scientific research considerations for managing the possible external variables that may affect the study results. Moreover, the nephrologist’s suggestions were also considered when the researcher selected these criteria to make the study program application appropriate and harmless.
Study procedures
All participants underwent the same evaluation and battery of tests;after a proper explanation of the test procedure,they were fully aware of the study’s goals and procedures, they agreed to participate in the current study, and they signed written informed consent at the beginning of this study, according to the ethical principles and guidelines for the protection of human subjects and approved by the institutional ethics committee of Faculty of Nursing, Kufa University.The protocol is registered at the International Clinical Trials Registry Platform (ICTRP) in World Health Organization (Registration Number IRCT20210312050679N1) to meet the International Committee of Medical requirements Research; additionally, it is considered to be a scientific, legal, ethical and moral responsibility.
Study instrument
The researcher adopted the instrument of study based on the previous scientific kinds of academic literature to investigate the study phenomenon. The questionnaire is related to the patients’ physical performance, the checklist of physiological parameters, and complications. The final copy consists of the following:
Part I Socio-demographic characteristics. This part involves socio-demographic data obtained from the patients undergoing hemodialysis using an interview. This part comprised 6 items, which included age, gender, body mass index, level of education,occupational status, and socioeconomic status (monthly income).Weight and height will be assessed by a portable stadiometer(Detecto’s ProMed 6129 medical scale, 203 E. Daugherty, Webb City,MO, USA).
Part II Clinical characteristics. The second part of the questionnaire concerns collecting clinical characteristics. Data will be obtained from the patients undergoing hemodialysis through the interview.This part is comprised of two subparts, which include past and present medical history and clinical assessment.
(1) Past history: Completely describing the complaint will be determined, and information on the patient’s medical history will be collected to provide necessary background information such as(diabetic Mellitus, coronary artery disease, hypertension, and others).(2) Present history: Investigated present medical history to elicit information about the presenting complaint. The present history form has chronic kidney disease-related problems and complications such as(anaemia, renal stone, etc.).
Part III evaluation of physical performance by (short physical performance battery) tool. There are many tools and approaches used to assess physical performance, such as (Fried’s criteria, Reuben“physical performance test”,and the Frailty index).But the researcher was chosen the Short Physical Performance Battery (SPPB) scale as a measure of performance based on physical ability because it has many advantages:
· Completed in just a few minutes, training required for administration was minimal, and the use of simple equipment was needed.
· In addition, results can be quantified by points and can be reproduced and adapted to the changes in functionality over time.
· The short physical performance battery can be safely used to evaluate functional capacity in outpatient and clinical settings.
· It can be useful in identifying activities of daily living (ADLs).
· It also predicts the risk of disability in older chronic disease patients hospitalized.
· The short physical performance battery tool is an objective measurement.
Jack Guralnik and colleagues developed the scale in 1994 as part of a National Institute on Aging project, the Established Populations for Epidemiologic Studies of the Elderly (EPESE). It has been used in large-scale epidemiological studies and, as such, has an excellent normative basis. The short physical performance battery is a well-established instrument for measuring physical performance,commonly used among community-dwelling adults, nursing home residents, and hospitalized patients [12]. The SPPB is an objective measure and a validated and reliable assessment tool for measuring lower extremity function that is widely used in both clinical and research settings.The SPPB comprises three parts:the balance test,the gait speed test,and the chair stand test[13].It can be shown clearly in(Figure 2).
Study instrument validity
The validity of an instrument concerns its ability to gather the data it intends to gather. The face validity of the nursing intervention program and the study instrument are determined through the use of a panel of (30) experts who have more than ten years of experience in their scientific field to review the nursing intervention program for it’s content, instrument, and investigation clarity, relevancy, and adequacy of the questionnaire to measure the concepts of interest.Moreover, an expert’s mean years of experience is 21.2 years. Some demographic and clinical items were deleted after a face-to-face or by e-mail discussion with each expert.After considering all the comments and recommendations of experts, the instrument will consider valid.
Method of data collection
The researcher will collect the data using the developed questionnaire and the structured interview technique with the subjects, who were individually interviewed using the questionnaire. The researcher will utilize face-to-face interviews for the socio-demographic and clinical data. Regarding the physical performance evaluation, the researcher will use the guided observation technique to evaluate the patients’physical performance through the short physical performance battery(SPPB) scale before and after the program’s application. The researcher assessed physiological parameters using the hospital tools to measure blood pressure (evaluated from the non-fistula arm) and checked heart rate, respiratory rate, and oxygen saturation by portable pulse oximeter for each patient to insure the standardization of these tools following established guidelines. Regarding the evaluation of the physical performance after the application of the SPPB for the study group, the researcher will use two evaluation periods (after eight weeks of the program application) while the following established guidelines closely monitor the patients. For the control group, the researcher will use a pre-test and two post-test evaluations without applying the resistance exercises training, and they still receive management routinely.
Materials will be used to collect objective data
The researcher will use the following materials in the present study:(a chair; stopwatch; stethoscope; portable stadiometer;sphygmomanometer; portable pulse oximeter fingertip; resistance elastic bands loop exercises; short physical performance battery test mobile application). These tools and devices will be used from the hospital;that is,they had calibrated,except SPPB, which is adapted to be valid and reliable tools.
Primary outcome measures
Outcome measures assessed change from baseline at eight weeks for the following: Short Physical Performance Battery (SPPB): A combination of physical tests that assess balance, gait speed, and lower limb functional strength that total score ranging from (0 worst to 12 best), each test was scored on a scale of (0 to 4 points) with using cut point criteria as follows: (0-6 points) low performance, (7-9 points) intermediate performance, and (10-12 points) high performance. Short physical performance batteries are widely used both in the clinical and research environment. It is also a validated low extremity function measurement for chronic kidney disease patients and predicts disability and mortality.
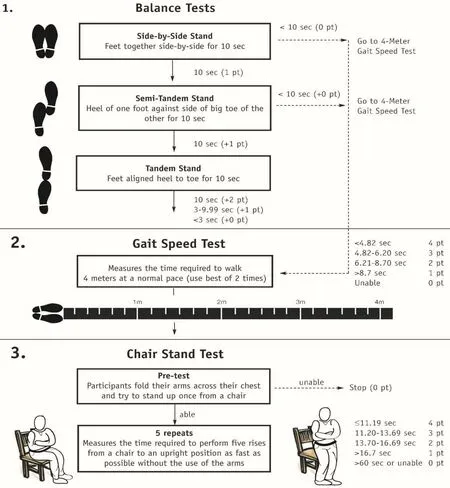
Figure 2 Flowchart for the short physical performance battery tool
Secondary outcome measures
Sit-to-stand-to-sit 10 and 60 tests (STS): Used for resistance and strength assessment, respectively, of the lower limbs' muscle capacity force. STS-10 is calculated as the total time needed to complete 10 consecutive repetitions of standing up and sitting down again,whereas the STS-60 registers the number of repetitions performed in 60 seconds. This test is easy, inexpensive, fast, reproducible, and is used in the test pack for renal diseases. The STS10 and STS-60 have been found to be valid measures of lower body muscle endurance force. The 6MWT is an indicator of the participant’s functional capacity, and it registers the maximum number of meters the participant is able to walk in a 30-m distance corridor.The 6MWT is a simple,valid tool for testing the ability to perform daily life activities,e.g., walking. And Physical Activity Scale for the Elderly (PASE)addressed the participant’s physical activity level.
Statistical analysis
Before statistical analysis, all continuous variables will be tested for statistical normal distribution using bar charts, the normal distribution curve, and the Shapiro-Wilk test. The following approaches to statistical data analysis will be used to analyze study data by applying Microsoft Excel (2016) and Statistical Package for the Social Sciences(SPSS)version 26. The analysis included two types of statistics; Descriptive Data Analysis: presented as Tables:Percentages, Frequencies, and Graphic presentation by using(Statistical figures). Statistical mean and standard deviation.Inferential Data Analysis: Statistical tests will be applied according to the distribution and type of variables. These will be used to accept or reject the null hypothesis, which includes the following:
An independent sample t-test will use to compare the means difference between two independent samples (study and control groups) to assess whether statistical evidence exists that the related population results vary significantly. The researcher will use paired t-test to determine the mean difference between the pre-test and post-test for the study and control groups.Will use a one-way Analysis of Variance (ANOVA) for pre-test and post-test1, and post-test2 for each group of physical performance outcome scores; a repeated measures analysis supplemented this.A Chi-square test will be used to compare frequencies for the goodness of fit and find out the association between different variables.
In the present study, the researcher will be depended on the confidence interval (0.99) to determine whether there will be a considered significant difference or correlation for the effectiveness of the program, while the (0.95) confidence interval will be used to investigate the effect of socio-demographic data and clinical characteristics on the implementation of the program.
Application of the intervention program
Steps of application to the program:
Because the program is designed within the conduct of nursing, its application has done theory of the Nursing process as follows:
1. Nursing assessment: This phase includes assessing the patient for demographic and clinical data about the End-stage kidney disease patients' physical activity through the physical performance that will be collected by the short physical performance battery (SPPB) test before the application of the program
2. Nursing diagnosis: In this phase determines, the following nursing diagnosis according to the data collected during the assessment step; the nursing diagnosis is (Impaired physical performance related to chronic kidney disease manifested by () scores).
3. Nursing planning: According to nursing diagnosis, the nurse should use the resistance exercise training program (Knee extension, Hip abduction, and Hip Flexion with Resistance Bands) as a physical rehabilitation technique plan.
4. Nursing implementation: implementation of a nursing care plan. Application of the designed program directly to the patients after the ethical considerations are achieved. Nurse will be using the resistance exercise training program for the patients to enhance their ability to physical performance it under the supervision of the researcher.The implementation process involved the application of the resistance exercises training program according to the following procedure:
· Assessment of physical performance by short physical performance battery: The SPPB test is divided into three parts:assessment of the balance test consisting of three subtests,a gait speed test, and the chair stand test. These subtests are to be conducted sequentially.
· The researcher simulates the resistance exercise training to the patients to enhance their ability to perform it. And the patients perform the resistance exercise under the researcher’s supervision.
· The researcher explains how the patients perform resistance exercise training later for follow-up. The patient can perform the exercise ranging from 3-10 times, with no medical limitation.
· A point system in which higher numbers mean the better output is chosen, with a maximum of 4 points to be obtained in each subtest.To go on to the next subtest,this limit must be reached.
· To achieve the full score of 4 points, patients need to complete all the repetitions successfully in the subtest. In total, 12 points are the highest score a patient can obtain, which denotes high physical performance.
Explanation of resistance exercise
A well-rounded fitness program includes strength training to improve joint function,bone density,muscle,tendon,and ligament strength,as well as resistance exercises to improve heart and lung fitness,flexibility, and balance exercises [14]. Resistance training is based on the principle that the body’s muscles work to overcome resistance forces when necessary [15]. The physiotherapist must ensure that the suggested exercises be individualized to the CKD patient’s current stage of physical ability to be done twice or thrice per week.Resistance strength will be set based on the Borg rating of perceived exertion, and rating 13 (somewhat hard) will be set as the targeted strength [16]. Proper breathing techniques will be emphasized during all exercises to avoid the Valsalva maneuver, as previous research recommends [17]. Training protocols consist of two sets of 10 repetitions of three resistance training types for lower extremities.:knee extension, hip abduction, and hip flexion using an elastic band(Thera-Band Resistance Band Loops, Thera-band, Ohio, USA)encircling both ankles or above the knees, in a sitting or supine position depending on patient preference or ability for three sessions per week.
Knee extension (leg extension): sit in a chair or supine position. Put one end of the resistance tape on your right knee and secure the other end on your left leg. Lift and put your right leg on the right, and hold it for a few seconds. Lower your knee. Repeat using your left leg. 8 to 10 times with each leg. You should feel all the muscles in the front of your thigh working. It will feel harder the higher you lift your foot[18]. Compensation: If the band is slipping, pull the band away from your ankle and cross the bands to form a loop. Put your toes through the loop to secure the band to your ankle[19] (Figure 2).

Figure 2 Knee extension with resistance band
Hip abduction: sit in a chair or supine position, depending on patient preference or ability. Wrap the resistance bands around the knees or ankles, extending the hip width of the knees. Slowly push your knees to the side, then return them to control and keep your feet together. Hold and slowly return. Repeat 8 to 10 times (Figure 3).
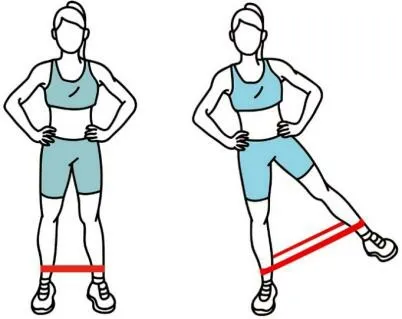
Figure 3 Hip abduction with resistance band
Hip flexion: To flex your knee, wrap the resistance band at the end of one end around your right ankle and the knee at the end, and then wrap the other end on your left ankle. Your right foot will be slightly elevated from the ground, the right knee will bend, and you will be able to move towards your stomach. Extend the right knee to the starting position. Repeat the exercise with the left leg when you finish the number of exercises on the right leg. Repeat 8 to 10 times (Figure 4).Progression was performed by increasing contraction time up to 6 seconds, and patients performed 1 set of 10 repetitions. As recommended by previous research, a proper breathing technique was emphasized during all exercises to avoid the Valsalva manoeuvre.

Figure 4 Supine hip flexion with resistance band
5.Evaluation: This process involved a re-assessment of the patients' physical performance using the scale and then comparing the scores of the physical performance ability after the program's application with the scores collected in the pre-test, which was determined through the assessment step before the application of the program.
Discussion
Low physical performance is a common complication associated with CKD; low physical performance and impairment are associated with elevated risks of disability and death. In addition, this concept has been expanded further to show that CKD is also associated with weak functional status. Physical activity is an important part of healthy lifestyles for all adults, especially the elderly. Most of the physical activity guidelines emphasise a 75-minute-a-week exercise to reduce the risk of chronic diseases. However, new evidence suggests that resistance training can effectively reduce the risk of many chronic diseases. The aim of this study is to study the effectiveness of resistance training in the physical performance of patients on hemodialysis. The theory of resistance exercise training should be an effective treatment for chronic kidney disease. However, the evidence of resistance exercise training is inadequate, and the effect of resistance exercise training exercise is disputed for chronic kidney disease. Researcher will perform a prospective, double-blind,randomized controlled trial of resistance exercise training for patients with chronic kidney disease and undergoing hemodialysis. Resistance exercise training could produce more beneficial effects than general exercise for chronic kidney disease and patients undergoing hemodialysis, reducing fatigue and improving function and quality of life.
Strengths and limitations
First, most of the previous resistance training studies were usually between several weeks and eight weeks. The study duration is an intervention period of 8 weeks and a follow-up period (with no active intervention) of 8 weeks, giving a total study period of 4 months.Second, in the present study, the intervention group performed three movements with resistance exercise, but the control group did not receive the exercise. On this basis, the study may reduce other prejudices compared to previous studies. Thirdly, earlier studies focused primarily on disabilities and quality of life. But physical performance is rarely analyzed for resistance exercise training on chronic kidney disease. There are also some limitations to this study,and the total number of participants is not large. (68 patients).
Moreover, only one exercise frequency is used to estimate the effect of resistance exercise training for chronic kidney disease patients, and different exercise frequency groups should be added to subsequent studies. Despite the well-known benefits, several barriers exist to implementing exercise routines within hemodialysis care. The current study may encounter some limitations, such as patients dropping out before the study is completed; perhaps, researchers cannot contact them regularly or are unaware of the factors of patient and comorbidity that may interfere with the study. Longer follow-up is needed to determine if these results will be interpreted into decreased death rates. Future research will attempt to overcome these limitations.
Finally,the aim of this study is to determine the impact of resistance training on chronic kidney diseases patient undergoing hemodialysis and estimate whether resistance exercise training has beneficial effects on general physical performance. The study’s results will benefit patients, researchers, and policymakers interested in treating patients with chronic kidney diseases. The results support the idea that exercise is more important, so we encourage therapists to implement exercise in their daily hemodialysis routine regardless of the resources they can count on.

- TMR Non-Drug Therapy的其它文章
- Active sham cupping therapy technique:identification of limitations and suggesting enhancements
- Effects of exercise-based cardiac rehabilitation on inflammatory biomarkers in patients with cardiovascular disease:a systematic review with meta-analysis
- The role of pain neuroscience education in the management of chronic musculoskeletal pain:a physiotherapeutic approach
- Implementation of alternative methods in the health system through evidence-based medicine