
Effect of internet multiple linkage mode-based extended care combined with in-hospital comfort care on colorectal cancer patients undergoing colostomy
2023-10-21 01:04LiXuMeiZhenZhou
Li Xu, Mei-Zhen Zhou
Abstract
Key Words: Ⅰnternet multiple linkage mode; Extended care; Ⅰn-hospital comfort care; Colorectal cancer patients; Patients undergoing colostomy
INTRODUCTION
Colorectal cancer refers to the malignancy occurring at the junction of the rectum and sigmoid colon and is the second most common gastrointestinal malignancy after gastric cancer. The main clinical manifestations of patients are mucousy and bloody stool, constipation and diarrhea. The incidence of colorectal cancer is related to diet, environment, genetics and other factors[1-3]. The 2018 Chinese cancer statistics showed that the incidence and mortality of colorectal cancer in China ranks fifth among all malignant tumors, including 376000 new cases and 191000 deaths[4].
At present, laparoscopic-assisted transabdominal perineal combined radical rectal resection (Miles operation) has the same indications as traditional laparotomy. Generally, tumors less than 5 cm away from the anal verge are surgically removed. This procedure requires a permanent colostomy in the left lower abdomen[5]. In China there are about 100000 new colostomy patients every year, and the cumulative number of colostomy patients has exceeded 1 million. It is expected that this number will continuously increase[6]. Permanent colostomy is required in 50%-60% of colorectal cancer patients[7]. The incidence of enterostomy complications abroad is 11%-60%, and the domestic literature reports 16.3%-53.8%[8]. Patients will lose their normal defecation ability and be unable to defecate independently. Additionally, the installation of an ostomy bag brings severe psychological pressure to patients, which causes anxiety, depression and other adverse emotions, affecting the prognosis of patients. Thus, it is of great significance to give scientific and effective care to patients with colorectal cancer[9].
Routine nursing refers to the normative regulations of nursing prevention and control measures formulated under the guidance of basic theory and combined with long-term clinical nursing practice experience[10]. For patients undergoing colostomy, routine care only meets basic needs. Comfort care is a new mode of nursing, which refers to a nursing method that encourages patients to the happiest mental, physical and socio-spirit state[11]. Due to the special situation of patients undergoing colostomy, sufficient nursing guidance should be paid not only during hospitalization but also after discharge to extend the nursing of patients from the clinic to the family and further improve the nursing effect[12-14].
Multiple linkage mode refers to the integration of hospital, community and family to avoid disjointed nursing intervention after discharge[15-17]. Internet-based continuous care has also been widely used in clinical practice. Recent studies have applied it to the care of adrenal tumor patients, and the nursing effect was good[18]. The present study explored the application effect of the internet-based continuous care mode hospital guidance-community participationfamily cooperation combined with in-hospital comfort care in patients undergoing colorectal cancer colostomy.
MATERIALS AND METHODS
General data
Data from 187 patients with colostomy who were treated in our hospital from May 2019 to March 2022 were collected and divided into three groups, A (n= 62), B (n= 62) and C (n= 63), according to different intervention methods. In group A, there were 39 males and 23 females. The ages ranged from 32 years to 68 years, with an average of 47.82 ± 5.42 years; 29 cases completed junior middle school or below, 27 cases completed technical secondary school/senior high school, and 6 cases completed junior college or higher. Patients were divided by Dukes stage as follows: 30 cases were in stage I; 24 cases were in stage II; and 8 cases were in stage III. Thirty-five cases were in ostomy stage II, and 27 cases were in ostomy stage III. In group B, there were 44 males and 18 females. The ages ranged from 30 years to 70 years, with an average of 48.15 ± 5.37 years; 26 cases completed junior middle school or below, 25 cases completed technical secondary school/senior high school, and 11 cases completed junior college or above. Patients were divided by Dukes stage as follows: 33 cases were in stage I; 21 cases were in stage II; and 8 cases were in stage III. Twenty-three cases were in ostomy stage II, and 39 cases were in ostomy stage III. In group C, there were 39 males and 24 females. The ages ranged from 28 years to 66 years, with an average of 47.36 ± 4.59 years; 32 cases completed junior middle school or below, 22 cases completed technical secondary school/senior high school, and 9 cases completed junior college or above. Patients were divided by Dukes stage as follows: 33 cases were in stage I; 23 cases were in stage II; and 7 cases were in stage III. Twenty-five cases were in ostomy stage II, and 38 cases were in ostomy stage III. The general data of the two groups were comparable (allP> 0.05). This study was approved by the ethics committee of the hospital.
Inclusion criteria
(1) Diagnosed with colorectal cancer by clinicopathological diagnosis; (2) Older than 18-years-old; and (3) Complete clinical case data.
Exclusion criteria
(1) Patients with severe physical dysfunction; (2) Patients with severe hearing impairment and visual impairment; (3) Patients with consciousness dysfunction; (4) Patients with palliative surgical resection; and (5) Patients with vascular dementia, mental disorders and disturbance of consciousness caused by stroke.
Methods
Group A received internet multiple linkage mode-based extended care combined with in-hospital comfort care. Group B received internet multiple linkage mode-based extended care. Group C received usual care intervention.
Group A: Group A was given internet multiple linkage mode-based extended care combined with in-hospital comfort care. Internet multiple linkage mode-based extended care was the same as group B and is described below. The details of in-hospital comfort care were as follows: (1) Creation of comfortable sickroom environment. Comfortable ward environment was created for patients to ensure adequate light and cleanliness in the ward, to ensure indoor quiet and to ensure that patients get comfortable sleep; (2) Psychological comfort care. Colorectal cancer patients with colostomy have great psychological pressure and emotional instability and are prone to irritability, fear and other adverse emotions. Nursing staff can take the initiative to provide psychological support for patients, chat with patients more and alleviate patients’ adverse emotions so patients can reach a comfortable state psychologically; (3) Pain care. Medical staff can explain the law of postoperative pain to patients, guide patients to distract themselves from the pain by listening to music and chatting with their families, evaluate the degree of pain and give painkillers appropriately; (4) Dietary care. The nursing staff should instruct the patients to avoid eating greasy, flatulent and crude fiber-rich foods, minimize the number and amount of defecation, protect the artificial anus, eat more foods with high protein, high vitamins and low fiber, eat on time and to not overeat; (5) Stoma comfort care. The patients were required to expose the stoma and clean the excrement from the stoma 2-3 d after the operation. Physiological saline was used to clean the skin around the stoma, and relevant skin care solution was used to protect the skin around the stoma and reduce fecal pollution; and (6) Rehabilitation comfort care. Medical staff should tell patients to wear loose and comfortable clothes and prevent friction stomatology. Patients should avoid water wetting their stomatology bags when bathing. They can cover the stomatology bags and replace the stomatology bags after bathing. They should regularly clean up excreta and make bags and put deodorant in the stoma bag to remove the smell.Group B: Group B was given internet multiple linkage mode-based extended care. An intervention group for colorectal cancer patients with colostomy based on internet + multiple linkage mode was established. One network engineer with more than 5 years of working experience and 15 medical oncology staff were selected to form the intervention group. The 15 medical staff included 2 attending doctors and 13 nurses. The 13 nurses included 1 chief superintendent nurse, 1 deputy chief superintendent nurse, 5 supervisor nurses and 6 nurses, all of whom had more than 6 years of ostomy nursing experience. The chief superintendent nurse was responsible for the overall guidance of the nursing process. The deputy chief superintendent nurse was responsible for the data-push and training of nursing knowledge. The supervisor nurses were responsible for the training and guidance of the nurses in the community hospital. They also cooperated with the network engineer to adequately design the network platform and update the push content, check and reply to the messages of patients and their families and collect background feedback. Among the 6 nurses, 4 were responsible for nursing training of family members and patients themselves, and the other 2 were responsible for collecting intervention data and sorting data.
The network engineer built a WeChat applet called “colorectal microplatform” and created patient communication groups. The applet included the medical side and the patient side. The medical side had three sections: information verification; health knowledge; and physician-patient interaction. Information verification was used to audit and verify the registration information of patients and their families. The health knowledge section aimed to collect videos, pictures and texts about colostomy nursing knowledge of colorectal cancer and push it three times a week for 1 mo. The content of the 1stweek included psychological counseling and ostomy bag replacement method. Physical needs included exercise, bathing, clothing, diet and sexual life and social interaction (traveling, working and gathering). The content of the 2ndweek included observation and prevention of the occurrence of ostomy complications, ostomy defecation and abdominal conditions, observation of local and surrounding skin conditions of ostomy, guidance of enterostomy methods and the time and method of the appointment of ostomy clinic review. After 1 mo, the above content can be sent repeatedly. In the physician-patient interaction section, daily observation records, message response and online follow-up can be viewed.
The patient side included the patient’s personal data, information platform and interaction. The personal data included the patient’s sex, age and other basic information as well as ostomy information. The information platform provided psychological and physiological knowledge of colorectal cancer ostomy. The interactive section provided the function of leaving messages in the background. Patients and their families can leave messages in the interaction section for consultation if they have any questions. Intervention group members checked background messages every day and answered them in time. Patients could also express their questions through WeChat group chat. The interaction section also included a service evaluation content, which enabled patients and their families to put forward opinions and suggestions to the interventionists and the platform, which was conducive to continuous improvement of the platform.
Group C: Group C was given usual care intervention. During the period of hospitalization, patients were instructed in routine daily behavior, and usual care was carried out according to the nursing method of enterostomy. The patient was instructed in a series of daily activities such as diet, exercise, washing, rest and defecation and was told to clean the enterostomy and surrounding skin. The emergency treatment measures for possible abnormalities after the completion of the enterostomy were explained. Appropriate psychological intervention was performed for patients with colostomy of colorectal cancer.
Observation targets
Baseline data, the occurrence of complications, the stoma self-efficacy scale (SSES)[19] rating, Hamilton Anxiety Scale (HAMA)[20], Hamilton Depression Scale (HAMD)[21], Brief Fatigue Inventory[22], City of Hope-Quality of life-Ostomy Questionnaire (COH-QOL-OQ)[23] were collected from all patients. Complications were compared among the three groups. The SSES, HAMA, HAMD and COH-QOL-OQ scores of the three groups were compared before and after intervention. SSES included two dimensions and six individual items, with a total of 28 items and a total score of 28-140 points calculated with a 5-point scoring system. The score of ostomy care efficacy was 13-65 points, and the score of social efficacy was 9-45 points. HAMA had 14 items in total, and the score was 0-4 with 5 grades. The total score was 0-56. The higher the score, the worse the anxiety symptoms. HAMD had 17 items in total, and the score was 0-4 with 5 grades. The total score was 0-68. The higher the score, the worse the depression symptoms. The Brief Fatigue Inventory consisted of nine items, which were scored on a scale of 0 to 10, including no fatigue (0), mild fatigue (1 to 3), moderate fatigue (4 to 6) and severe fatigue (7 to 10). COH-QOL-OQ included four dimensions with a total of 32 items: physical health (11 items); psychological health (9 items); social health (7 items); and mental health (5 items) It adopted the scoring method of 0-10 points, and the total score was 0-320 points. The higher the score, the worse the quality of life.
Statistical methods
SPSS 11.0 statistical software was used to analyze and process the obtained data, and the measurement data was expressed as (x±s). Independent samplettest was used for inter-group comparison, and pairedttest was used for intragroup comparison before and after intervention. Counting data were expressed as frequency and constituent ratio.χ2test or Fisher exact probability method was used to compare disordered classification data, and rank sum test was for ranked data.P< 0.05 indicated that the difference was statistically significant.
RESULTS
Comparison of complication rate among the three groups
The complication rate in group A, B and C (16.13%, 20.97% and 60.32%) was significantly different (allP< 0.05). The complication rate in groups A and B was lower than that in group C, and there was no significant difference between groups A and B (allP> 0.05, Table 1).
Comparison of self-efficacy among the three groups
Before intervention, there were no significant differences in stoma care, social contact, diet choice, confidence in maintaining vitality, confidence in stoma self-care, confidence in sexual life, confidence in sexual satisfaction and confidence in physical labor among the three groups (allP> 0.05). After intervention, the scores of stoma care, social contact, diet choice, confidence in maintaining vitality, confidence in stoma self-care, confidence in sexual life, confidence in sexual satisfaction and confidence in physical labor in the three groups were all higher than before intervention. The scores of groups A and B were higher than those of group C (allP> 0.05, Table 2).
Comparison of anxiety and depression among the three groups
Before intervention, there were no significant differences in HAMA and HAMD scores among the three groups (allP> 0.05). After intervention, the HAMA and HAMD scores of the three groups were lower than before intervention. The scores of groups A and B were lower than that of group C. The scores of group A were lower than that of group B (allP< 0.05, Table 3).
Comparison of cancer-induced fatigue among the three groups
There were significant differences in cancer-induced fatigue among the three groups (allP< 0.05, Table 4).
Comparison of quality of life among the three groups
Before the intervention, there were no significant differences in the scores of physical health, psychological health, social health and mental health among the three groups (allP> 0.05). After the intervention, the scores of physical health, psychological health, social health and mental health of the three groups were lower than before the intervention. The scores of group A and B were lower than group C. The scores of group A were lower than group B (allP< 0.05, Table 5).
DISCUSSION
The main clinical treatment for colorectal cancer is surgical resection, but patients often need to perform ostomy after resection to promote the discharge of intestinal contents to protect the distal intestinal anastomosis and promote the recovery of intestinal diseases. Although ostomy can save the lives of patients, it violates the objective laws of the human body and can lead to the abnormal excretion pathway of patients, increase the psychological burden of patients and cause anxiety and depression in patients. Therefore, it is very important to provide long-term care in and out of the hospital for patients with colorectal cancer after ostomy[24-26].
Internet + mode is a new nursing mode that has emerged in the era of big data. The multiple linkage mode of the internet breaks the limitation of conventional nursing time and space, expands the scope of nursing services and can meet the health needs of patients at multiple levels. The use of information can encourage a close relationship between the hospital and patients, timely monitoring of the patients’ conditions and promotion of patient recovery. This study integrated the multiple linkage cooperation mode into nursing work. Information sharing and maintenance reminders were carried out through an internet platform, and hospital-community-home nursing was linked to provide comprehensive extended care for patients with colorectal cancer colostomy[27,28]. In-hospital comfort care is a humanized nursing measure, whose intervention aims to reduce patient discomfort, promote patient physical and mental comfort and ultimately promote patient postoperative recovery[29].
In this study, group A adopted the internet-based multiple linkage mode combined with in-hospital comfort care intervention, group B adopted the internet-based multiple linkage mode intervention, and group C adopted routine intervention. The results showed that the incidence of complications in groups A and B was lower than that in group C, and that no significant difference was seen between groups A and B. Intervention based on the multiple linkage mode of internet could effectively reduce the incidence of complications in colorectal cancer patients with colostomy. Complications of enterostomy patients may lead to the inability of the stoma bag to effectively collect excreta, seriously affecting patient emotions. In the intervention scheme based on internet multiple linkage mode, patients with abnormal conditions when dealing with the stoma can contact the medical staff through the WeChat platform, and the nursing staff can provide intervention support as soon as possible, effectively reducing the incidence of complications.
After intervention, scores of self-efficacy in groups A and B were significantly higher than those in group C, indicating that intervention based on internet multiple linkage mode can effectively improve self-efficacy in colorectal cancer patients with colostomy. This scheme pushed colostomy knowledge through the WeChat applet and provided colostomy patients and their families with colostomy-related medical knowledge by means of pictures and texts, which promoted colostomy patient understanding of their own state. By applying the knowledge learned in the WeChat applet to daily life, patients also further deepened their impression of colorectal cancer ostomy knowledge. Related psychological counseling pictures and texts in the information section were also conducive to improve patient confidence in treatment, and patient self-efficacy was significantly improved.
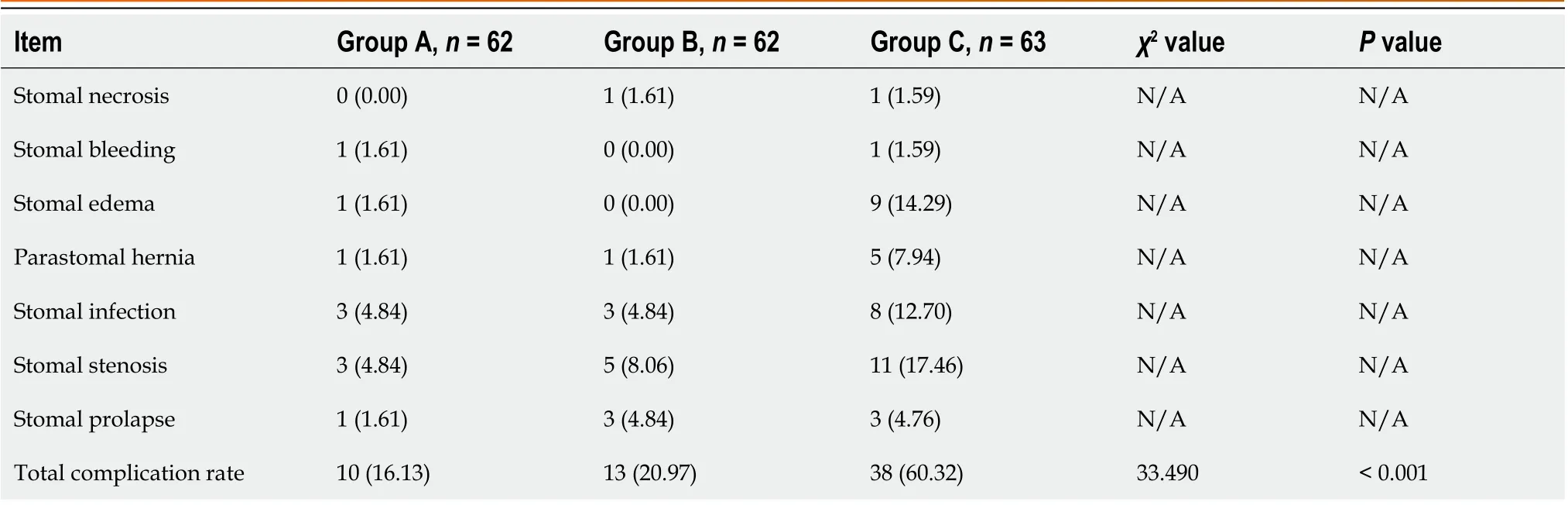
Table 1 Comparison of complication rate among the three groups
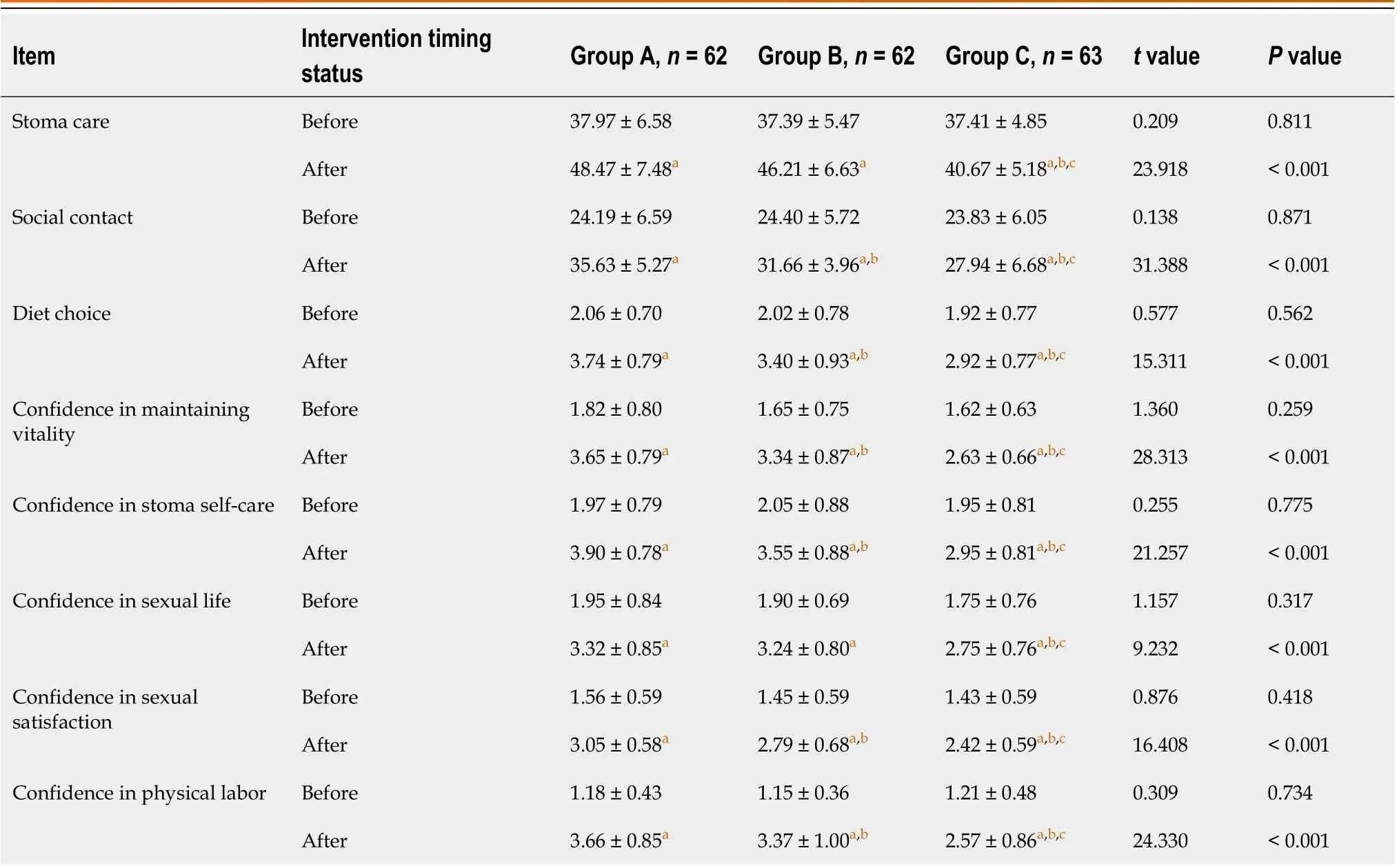
Table 2 Comparison of self-efficacy among the three groups
The HAMA and HAMD scores after intervention of the three groups were lower than before intervention. After intervention, the scores of groups A and B were lower than that of group C, and the score of group A was lower than that of group B. This showed that internet multiple linkage mode-based care combined with in-hospital comfort care can effectively improve anxiety and depression conditions in colorectal cancer patients with colostomy. Internet-based multimode intervention enabled patients to feel the support and care from medical staff all the time, shortened the distance between doctors and patients and nurses and patients and helped patients correctly face anxiety and depression. The WeChat public platform had message function, and medical staff encouraged patients through this board to relieve patient anxiety and depression symptoms. In-hospital comfort care enables patients to feel the care from medical staff through the creation of a comfortable ward environment, psychological comfort nursing, pain nursing, diet nursing and stoma comfort nursing. Thus, patient anxiety and depression were significantly improved, and the improvement of group A was better than group B and C.

Table 3 Comparison of anxiety and depression among the three groups

Table 4 Comparison of cancer-induced fatigue among the three groups

Table 5 Comparison of quality of life among the three groups
After intervention, the cancer-induced fatigue condition in group A was better than that in group B and group C, the scores of quality of life in groups A and B were lower than that in group C, and the scores of quality of life in group A were lower than that in group B. These results showed that internet-based multi-linkage model intervention combined with in-hospital comfort care can effectively relieve the cancer-induced fatigue and improve the quality of life of colorectal cancer patients with colostomy. The multiple linkage mode of the internet provided extended care through the WeChat platform, which not only provides health information but also includes communication with medical staff to answer questions, which allows patients to receive professional guidance more conveniently. In-hospital comfort care pays more attention to the physical and mental comfort of the patient and adopts a variety of measures to promote physical and mental comfort. The combined application of the two schemes further improved the cancer-related fatigue state and quality of life.
This study also had certain shortcomings. The sample size of this study was small, and it was a single-center study. In the future, a multi-center study will be undertaken to expand the sample size to ensure the accuracy of this study.
CONCLUSION
The application of extended care based on internet multiple interaction mode combined with in-hospital comfort care in patients with colorectal cancer colostomy can effectively reduce the occurrence of complications, improve their selfefficacy, relieve their cancer-induced fatigue and improve their quality of life, showing clinical application value.
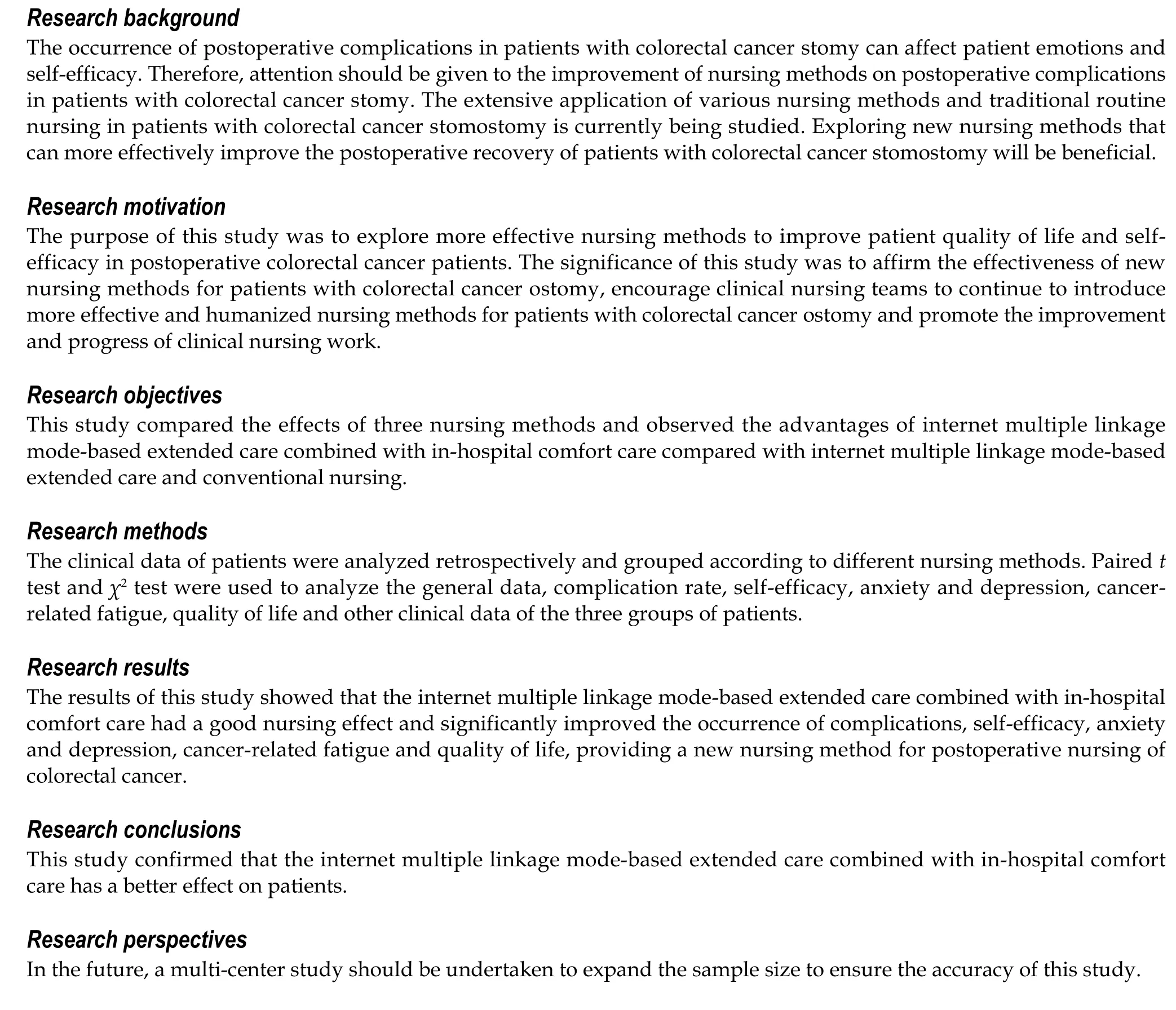
ARTICLE HIGHLIGHTS
FOOTNOTES
Author contributions:Xu L initiated the project and designed the experiment, conducted clinical data collection and performed postoperative follow-up and recorded data; Zhou MZ conducted a number of collation and statistical analysis, wrote the original manuscript and revised the paper; Both authors reviewed and approved the paper; All authors read and approved the final manuscript.
Supported byClinical Teaching Base of Jiangsu Medical Vocational College, No. 20219141.
Institutional review board statement:This study was approved by the Ethics Committee of People’s Hospital of Dongtai City.
Informed consent statement:The study was approved by the institutional review board at each participating site. The data are anonymous, and the requirement for informed consent was therefore waived.
Conflict-of-interest statement:The authors declare having no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Data sharing statement:All data generated or analyzed during this study are included in this published article.
Open-Access:This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers. It is distributed in accordance with the Creative Commons Attribution NonCommercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: https://creativecommons.org/Licenses/by-nc/4.0/
Country/Territory of origin:China
ORCID number:Mei-Zhen Zhou 0000-0001-8178-5070.
S-Editor:Fan JR
L-Editor:Filipodia
P-Editor:Cai YX
 World Journal of Gastrointestinal Surgery2023年9期
World Journal of Gastrointestinal Surgery2023年9期
- World Journal of Gastrointestinal Surgery的其它文章
- Preoperative and postoperative complications as risk factors for delayed gastric emptying following pancreaticoduodenectomy: A single-center retrospective study
- Comparative detection of syndecan-2 methylation in preoperative and postoperative stool DNA in patients with colorectal cancer
- Preoperative prediction of microvascular invasion in hepatocellular carcinoma using ultrasound features including elasticity
- Surgical management of gallstone ileus after one anastomosis gastric bypass: A case report
- Hepatic ischemia-reperfusion syndrome and its effect on the cardiovascular system: The role of treprostinil, a synthetic prostacyclin analog
- Advances and challenges of gastrostomy insertion in children