
Diagnostic performance of intravascular ultrasound-based fractional flow reserve in evaluating of intermediate left main stenosis
2024-03-26 02:38YongGangSUIChengYANGChangDongGUANYanLuXUNaQiongWUWeiXianYANGYongJianWUKeFeiDOUYueJinYANGShuBinQIAOWeiYUBoXUShengXianTUJieQIAN
Journal of Geriatric Cardiology 2024年1期
Yong-Gang SUI,Cheng YANG,Chang-Dong GUAN,Yan-Lu XU,Na-Qiong WU,Wei-Xian YANG,Yong-Jian WU,Ke-Fei DOU,Yue-Jin YANG,Shu-Bin QIAO,Wei YU,Bo XU,4,Sheng-Xian TU,Jie QIAN,?
1. Department of Cardiology,Fuwai Hospital,National Center for Cardiovascular Diseases,Chinese Academy of Medical Sciences and Peking Union Medical College,Beijing,China;2. Catheterization Laboratories,Fuwai Hospital,National Center for Cardiovascular Diseases,Chinese Academy of Medical Sciences and Peking Union Medical College,Beijing,China;3. Biomedical Instrument Institute,School of Biomedical Engineering,Shanghai Jiao Tong University,Shanghai,China;4. National Clinical Research Center for Cardiovascular Diseases,Beijing,China
ABSTRACT BACKGROUND The recently introduced ultrasonic flow ratio (UFR),is a novel fast computational method to derive fractional flow reserve (FFR) from intravascular ultrasound (IVUS) images.In the present study,we evaluate the diagnostic performance of UFR in patients with intermediate left main (LM) stenosis.METHODS This is a prospective,single center study enrolling consecutive patients with presence of intermediated LM lesions(diameter stenosis of 30%-80% by visual estimation) underwent IVUS and FFR measurement.An independent core laboratory assessed offline UFR and IVUS-derived minimal lumen area (MLA) in a blinded fashion.RESULTS Both UFR and FFR were successfully achieved in 41 LM patients (mean age,62.0 ± 9.9 years,46.3% diabetes).An acceptable correlation between UFR and FFR was identified (r=0.688,P < 0.0001),with an absolute numerical difference of 0.03(standard difference: 0.01).The area under the curve (AUC) in diagnosis of physiologically significant coronary stenosis for UFR was 0.94 (95% CI: 0.87-1.01),which was significantly higher than angiographic identified stenosis > 50% (AUC=0.66,P < 0.001)and numerically higher than IVUS-derived MLA (AUC=0.82;P=0.09).Patient level diagnostic accuracy,sensitivity and specificity for UFR to identify FFR ≤ 0.80 was 82.9% (95% CI: 70.2-95.7),93.1% (95% CI: 82.2-100.0),58.3% (95% CI: 26.3-90.4),respectively.CONCLUSION In patients with intermediate LM diseases,UFR was proved to be associated with acceptable correlation and high accuracy with pressure wire-based FFR as standard reference.The present study supports the use of UFR for functional evaluation of intermediate LM stenosis.
Adequately management of left main (LM)coronary artery stenosis is crucial given its higher perfusion responsibility for the left ventricular.[1]Previous studies have proved that revascularization by coronary artery bypass grafting (CABG) or percutaneous coronary intervention (PCI) for significant LM stenosis offers survival advantages over medical therapy,[2,3]while there is still controversial for the optimal treatment strategy of the mild or moderate LM stenosis.In clinical practice,revascularization treatment for intermediate LM lesions usually be chosen for the fear of undertreatment especially when the patients received surgical procedure.However,it is conceivable that an unnecessary stent implantation or an early operation usually with hardly benefit or even cause harmful prognosis to the patients.[4-6]Thus,to overcome this distinct clinical challenge,accurately evaluation of those LM stenosis is critical.
Although invasive coronary angiography has been considered as gold standard to assess lesion severity,it sometimes is believed lack of reliability especially when the LM diseases is involved.[7,8]In order to promote precise therapeutic strategies,physiological assessment or intravascular imaging assessment provided alternative modality for the evaluation of the intermediate LM coronary stenoses.[9-12]But all those lesion evaluation methods require special instruments,which makes it less realistic to perform both physiological and intravascular imaging assessment for the same patient in clinical practice from the safety concern or an economic viewpoint.The recently introduced intravascular ultrasound(IVUS)-based fractional flow reserve (FFR),denoted as ultrasonic flow ratio (UFR),is a novel fast computational method to derive FFR from IVUS images.[13,14]Previous study has proved high correlation and agreement between UFR and FFR in identifying functional significant coronary stenosis.[13]While the diagnostic performance of UFR in identifying functional significant intermediate LM stenosis,particular lesion subset with two downstream vessels,with FFR as a gold standard haven’t been evaluated to date.The goal of the present study is to determining diagnostic accuracy of UFR in patients with intermediate LM stenosis.
METHODS
Study Design and Population
This is a prospective,single center study designed to evaluate the diagnostic performance of UFR in identifying hemodynamically significant LM stenosis as compared with IVUS-derived minimal lumen area (MLA) with pressure wire-based FFR as the standard reference.Patients were eligible if they were ≥18 years old presented with intermediated LM lesions(diameter stenosis of 30%-80% by visual estimation);no restriction was placed on total diseased lesion number.Patients with stenotic lesions located in left anterior descending (LAD) or the left circumflex (LCx)coronary artery should undergo complete revascularization before FFR or IVUS assessment.Distal stenotic lesions were evaluated using visual estimation,only with no stenotic lesion or receiving successful treatment with no residual restenosis in downstream vessels,the patients would be included in the present study.Exclusion criteria were known intolerance to contrast agent or adenosine,in-stent restenotic LM lesion,severe heart failure,a serum creatinine level > 150 mmol/L,or a glomerular filtration rate <45 mL/kg per 1.73 m2;or other reasons that result in ineligibility for FFR,IVUS or UFR examination.
The study was designed by principal investigators,performed in compliance with the Declaration of Helsinki and approved by the ethics committee at Fuwai hospital.All eligible patients provided written informed consent.
Coronary Angiography and PCI Procedure
Standard angiogram acquisition was performed for LM and other vessels.Typically,nitroglycerin injection was recommended to eliminate arterial spasm;inject contrast till the distal downstream vessels are filled;and two angiographic images with at least 25°angles separation are recommended to fully display LM stenosis.LM lesion stenosis were visually estimated by each operator.Imaging or guiding catheter choosing were left to operator’s discretion.
Once there were significant lesions located downstream LM vessels (LAD or LCx),a PCI procedure with either balloon angioplasty or stent implantation would be performed according to standard practice.Only with no stenotic lesion or receiving successful treatment with no residual restenosis in LAD or LCx vessels,the patients would be included in the present study.After IVUS and FFR evaluation,the results would be reported to the operator separately,and the decision whether performed further treatment for those intermediate LM lesions were based on FFR results according to recent guideline.
IVUS Measurement
IVUS was performed when no stenotic lesion located in downstream vessels was confirmed using commercially available IVUS system (OptiCross,Boston Scientific,Boston,MA).The imaging run was performed using automatic pullback at a speed of 0.5 mm/s and recorded starting at the point distal to the LAD or LCx artery till aorta ostium.The choice of LAD or LCx artery was based on LM lesion extension.Usually,distal IVUS examination started from the downstream vessel with plaque extended;or recorded twice from both side branch artery once the narrowing lesions involved ostial of both LAD and LCx.To make the evaluated segment consistent between UFR and FFR,the distal point was settled accordingly to the intended distal location of FFR pressure wire.
After procedure,IVUS imaging were collected and send to the independent imaging core laboratory (Shanghai Jiao Tong University-Pulse Medical Imaging Technology Joint Laboratory) for offline UFR and quantitative IVUS measurement (MLA,plaque burden,etc.) blinded to FFR results.
FFR Measurement
FFR measurement was performed by operators in catheterization laboratory using RadiAnalyzer Xpress instrument and Certus pressure wire (St.Jude Medical,St.Paul,Minnesota).For all cases,pressure guidewire was introduced into the downstream coronary artery (LAD or LCx).Maximal hyperemia was induced by intravenous administration of adenosine-5’-triphosphate (ATP) at ≥ 160 mg/L per minute via the antecubital vein.The pressure recording was started for at least 10 s of stable value with hyperemia,and the pressure sensor was pulled back to the catheter tip to exclude pressure drift.
UFR Computation
The UFR analyses were performed by independent analysts blinded to FFR results using IvusPlus system (Pulse Medical Imaging Technology,Shanghai,China).The detailed methods for UFR calculation were described previously.[13]In brief,after analysts delineated the IVUS images to be analyzed,the UFR pullback could be obtained by the system automatically.During the calculation process,manual correction was allowed if border of lumen contours,external elastic lamina (EEL) and reconstructed side branches areas were recognized uncorrected.If the plaque extended to both LAD and LCx artery,two sequence of IVUS images from distal LAD to LM and distal LCx to LM would be transmitted for UFR computation separately.
Endpoints
The primary endpoint was receiver-operating curves (ROC) of offline UFR to identify hemodynamically significant LM intermediate stenosis with FFR as reference.Secondary endpoints including diagnostic accuracy,sensitivity,specificity,positive predictive value (PPV),negative predictive value(NPV),positive likelihood ratio (+LR),and negative likelihood ratio (-LR) for offline UFR,IVUS quantitative measurement (MLA) in identifying hemodynamically significant LM intermediate stenosis with FFR as the reference standard.
Statistical Analysis
The primary and secondary endpoints were analyzed based on patients with both UFR and FFR assessed.The data were analyzed based on patient level,the downstream vessel with lower FFR or UFR value was chose for final analysis,once the LM plaque involved both LAD and LCx resulting 2 pullbacks (distal LAD to LM and distal LCx to LM) for UFR and FFR.
Categorical variables are reported as percentage(counts) and continuous data are presented as mean± SD.The two-sided 95% CIs of diagnostic accuracy of offline UFR and MLA,with the FFR as the reference standard,were estimated at patient levels by using the Clopper-Pearson exact method.Using FFR as the reference standard,the relatedPvalue and two-sided 95% CIs of the difference on accuracy,sensitivity,specificity,NPV,and PPV between UFR and MLA were estimated.The ROC of UFR and MLA were estimated by using a logistic regression model.Correlation between UFR and FFR was determined by Pearson’s correlation coefficient (r).To compare the diagnostic performance of UFR and MLA,a cutoff value of ≤ 0.80 was used for both FFR and UFR to define the physiological significance of coronary stenosis.Cutoff values of both 4.5 mm2 and 6.0 mm2were chosen for MLA based on previous studies to predict functionally significant stenosis.All statistical analyses were performed with a test significance level of 0.05 using SAS version 9.4 (SAS Institute,Inc.).
RESULTS
Baseline Characteristics
Between March 2022 and November 2022,a total of 46 patients with intermediate LM lesions were screened.Finally,a total of 41 patients were enrolled(Figure 1).As shown in Table 1,the mean age of the patients was 62.0 ± 9.9 years,85.4% were men,46.3% with diabetes,and 58.5% patients presented with unstable angina.In 12 (29.3%) patients,LM lesion located in ostium;and LM bifurcation lesions occurred in 18 (43.9%) patients.Mean reference vessel diameter of LM lesion was 4.64 mm,average diameter stenosis was 66.2% (Table 2).
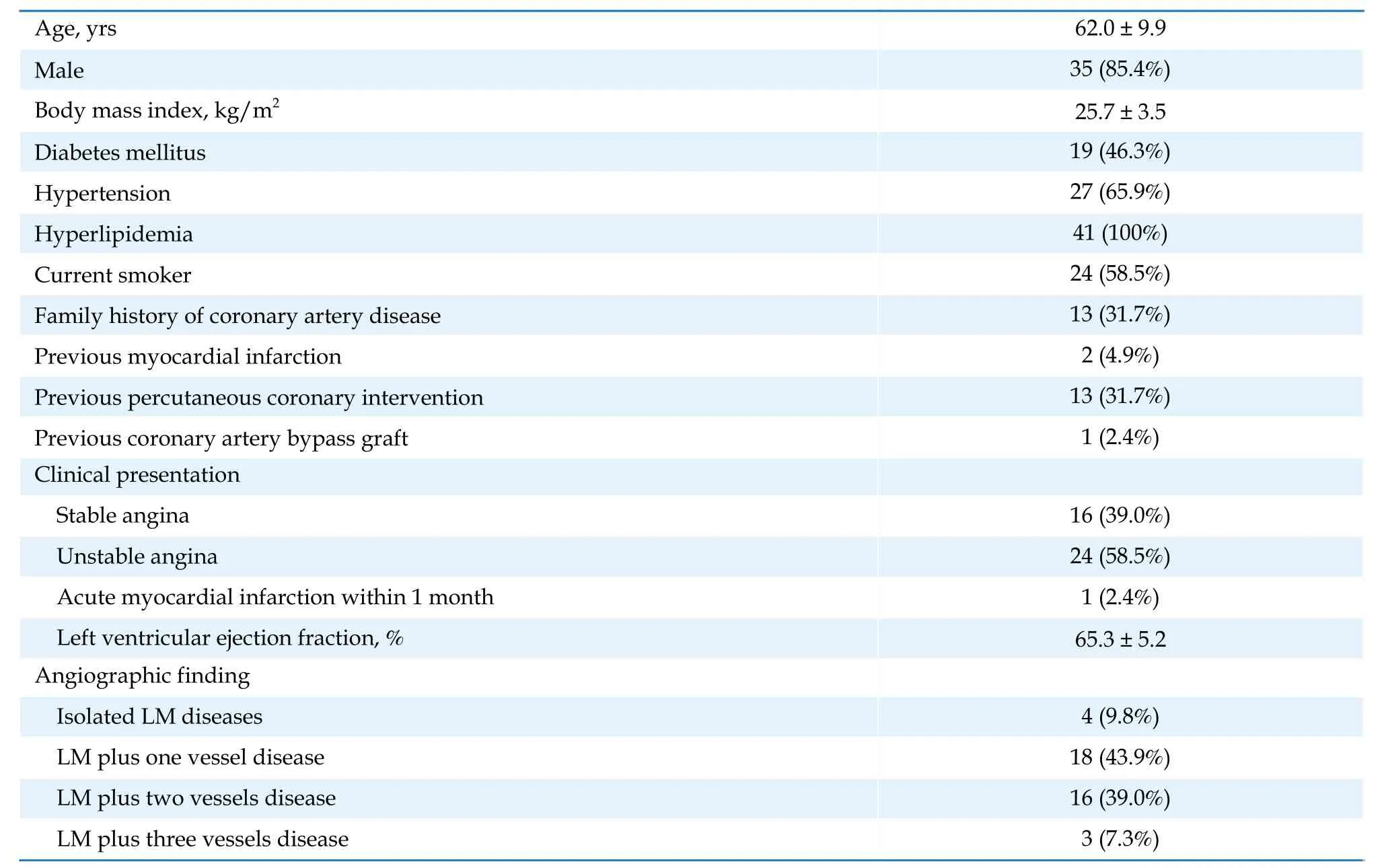
Table 1 Baseline patient demographics.
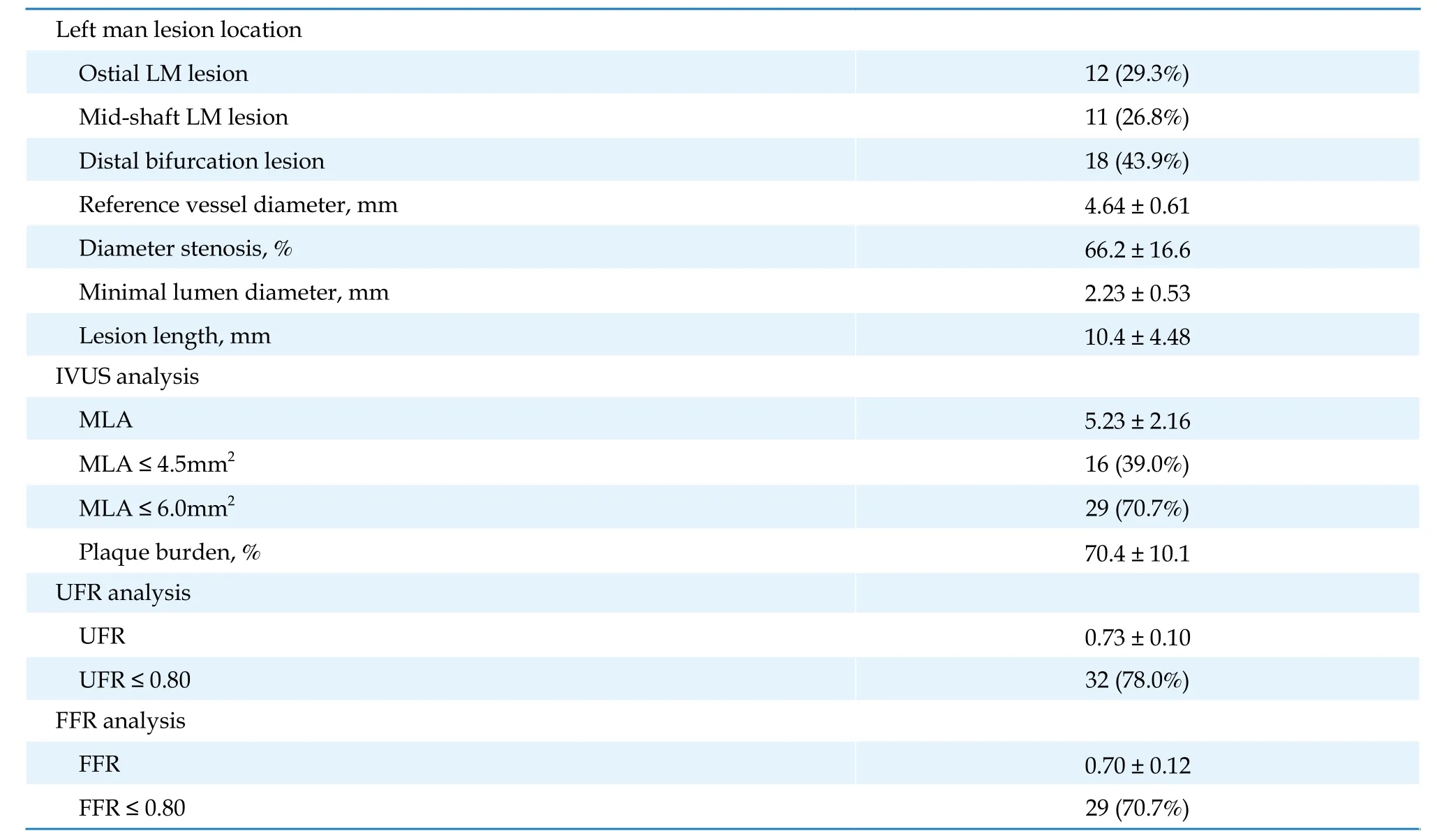
Table 2 Angiographic characteristics.
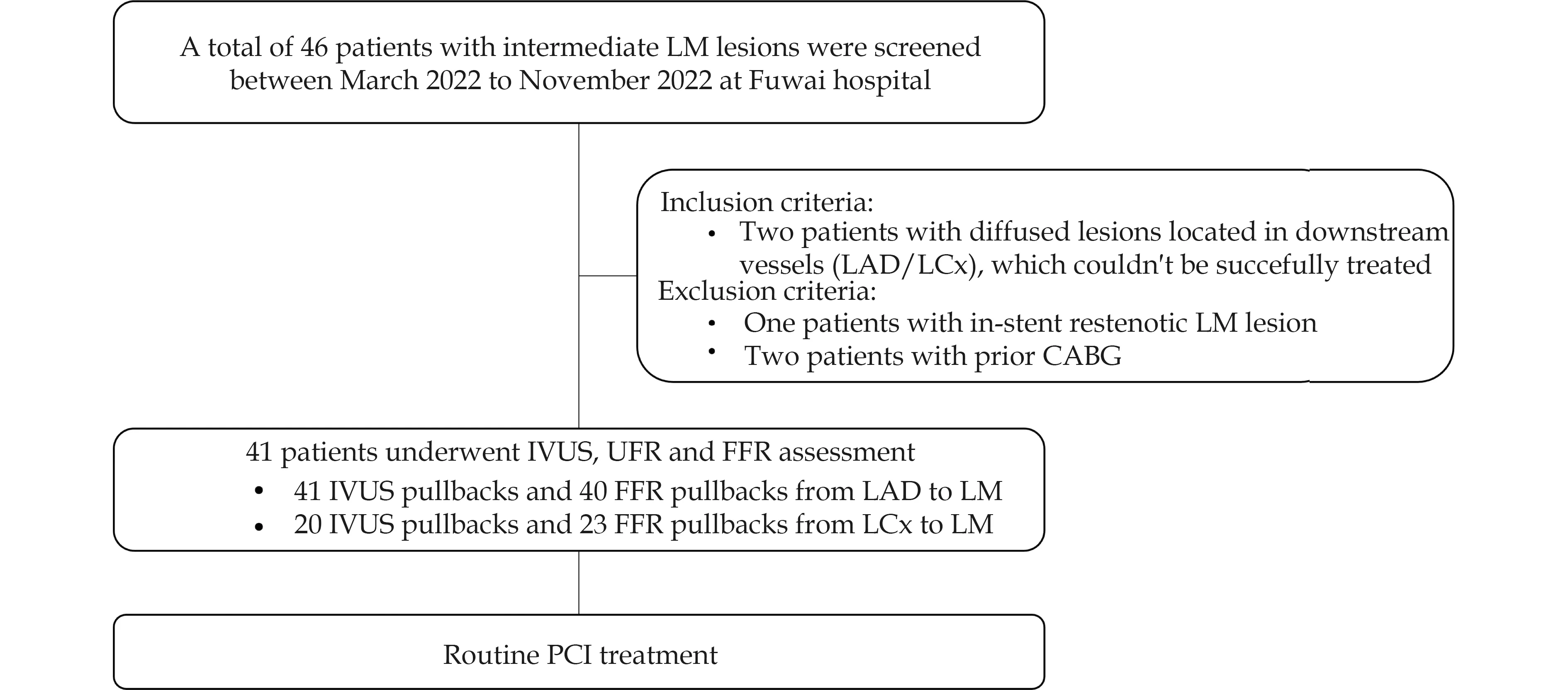
Figure 1 Study flow chart. CABG: coronary artery bypass grafting;FFR: fractional flow reserve;IVUS: intravascular ultrasound;LAD: left anterior descending;LCx: left circumflex;LM: left main;UFR: ultrasound flow ratio.
IVUS were successfully achieved in all 41 patients with 61 pullbacks (41 from distal LAD to LM and 20 from distal LCx to LM).Off-line UFR assessment based on IVUS imaging were successfully assessed in all 61 pullbacks.FFR measurement were succussed in all patients with 40 pullbacks from distal LAD to LM,and 23 pullbacks from distal LCx to LM.The mean FFR value was 0.70,and 29 (70.7%) patients were identified with functional ischemia.According to IVUS assessment,mean MLA was 5.23 mm2,among them 16 (39.0%) patients with MLA ≤4.5 mm2and 29 (70.7%) patients MLA ≤ 6.0 mm2.
Correlation and Agreement Between UFR and FFR
As shown in Figure 2,an acceptable correlation between UFR and FFR was identified in 41 patients(r=0.688,P< 0.0001).The absolute numerical difference between UFR and FFR was 0.03 (standard difference: 0.01),with an acceptable agreement between UFR and FFR (P=0.02).
Diagnostic performance of UFR and MLA
As shown in Figure 3,the area under the curve (AUC)in diagnosis of physiologically significant coronary stenosis for UFR was 0.94 (95% CI: 0.87-1.01),which was significantly higher than angiographic identified lesion diameter stenosis (AUC=0.66,P< 0.001)and numerically higher than IVUS-derived MLA(AUC=0.82;P=0.09).According to the receiver characteristic curve,best cutoff value of MLA for identifying functionally significantly LM stenosis was 6.10 mm2in the present cohort.
Per-patient level diagnostic accuracy of UFR was 82.9% (95% CI: 70.2-95.7),which was significantly higher than MLA when using 4.5 mm2as the treatment cutoff value (accuracy: 58.5 [95% CI: 42.2-74.8];difference: 24.4 [95% CI: 5.7-43.1],P=0.01).But was similar when using 6.0 mm2as the cutoff value (accuracy: 80.5 [95% CI: 67.1-93.8];difference: 2.4 [-14.4 to 19.3],P=0.78).
Diagnostic sensitivity was significantly higher with UFR as compared with MLA with 4.5 mm2as cutoff value (93.1%vs.48.3%;difference: 44.8 [95% CI: 24.2-65.4],P< 0.0001),but was similar when using 6.0 mm2as the cutoff value (93.1vs.86.2;difference: 6.9[95% CI: -10.2 to 24.0],P=0.43).Specificity,positive predictive value,negative predictive value,positive likelihood ratio,and negative likelihood ratio for UFR to identify FFR ≤ 0.80 was 58.3% (95% CI:26.3-90.4),84.4% (95% CI: 70.2-98.5),77.8% (95% CI:45.1-100.0),2.23 (95% CI: 1.14-4.40),0.12 (95% CI:0.03-0.49),respectively (Table 3).
FFR/UFR/IVUS Concordance
Figure 4 shows the four groups according to concordant and discordant FFR and UFR measurements,as well as the agreement with IVUS MLA significance (cutoff of ≥ 4.5 mm2or cutoff of ≥ 6.0 mm2).When using cutoff of 4.5 mm2,in MLA ≤ 4.5 mm2group (n=16,39.0%),14 patients (87.5%) had FFR ≤ 0.80,and 16 (100%) patients had UFR ≤ 0.80;while in MLA >4.5 mm2group (n=25,61.0%),10 patients (40.0%)had FFR > 0.80,and 9 (36.0%) patients had UFR >0.80.When MLA was ≤ 6 mm2(n=29,70.7%),25 patients (86.2%) had FFR ≤ 0.80,and 26 patients (89.7%)had UFR ≤ 0.80;while,when MLA was > 6 mm2(n=12,29.3%),8 patients (66.7%) had FFR > 0.80,and 6 patients (50%) had UFR > 0.80.
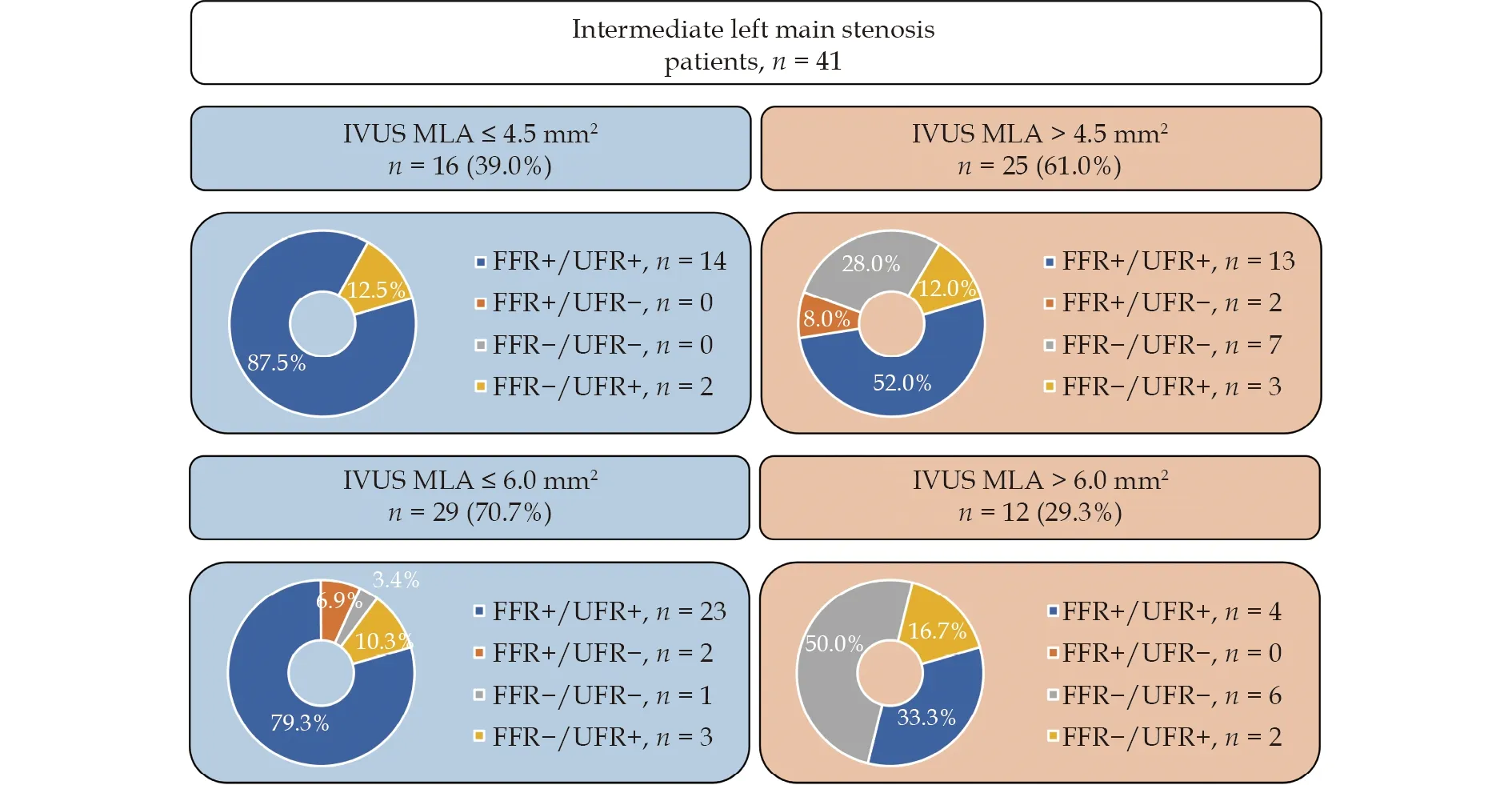
Figure 4 Proportion of patients with or without functionally significant LM stenosis identified by FFR or UFR as stratified by IVUS-derived MLA. FFR+denoted FFR ≤ 0.80;FFR-denoted FFR > 0.80;UFR+denoted FFR ≤ 0.80;UFR-denoted FFR > 0.80.FFR:fractional flow reserve;MLA: minimal lumen area;UFR: ultrasound flow ratio.
DISCUSSION
The present prospective,single center study enrolling consecutive patients with intermediate LM coronary stenosis demonstrated that: (1) UFR was associated with acceptable correlation and good agreement with pressure wire-based FFR as standard reference.(2) Using the conventional cutoff value of 0.80,UFR demonstrated a higher accuracy as compared with traditional IVUS-derived MLA when using 4.5 mm2as the cutoff value of in identifying hemodynamically significant LM stenosis with FFR as a standard reference;but showed similar accuracy and sensitivity when using 6.0 mm2as the cutoff value for MLA.
Assessment of Intermediate LM Stenosis
It has been proved that coronary angiography has several shortcomings in terms of interpretation of LMCA stenosis from a clinical standpoint,not only the challenge of precisely estimating of stenosis severity,but also the difficulty of identifying true extent of plaque burden.[15,16]Recent guidelines introduced intravascular imaging as well as physiological assessment,which have distinct strengths in guiding LM PCI.[17]Although in the fundamental trials DEFER[18]and FAME (Fractional Flow Reserve versus Angiography for Multivessel Evaluation),[19]LM coronary artery disease was excluded,the well-established “goldstandard” approach FFR has nevertheless been used for decision-making process regarding intermediate LM coronary artery stenosis.With FFR guidance,a better prognosis in LM patients has been demonstrated in several studies.[20,21]Meantime,IVUS has been widely used in the assessment of intermediate LM lesions for detailed anatomical information regarding the lumen,vessel,and plaque.The LITRO study (Prospective Use of an Intravascular Ultrasound-Derived Minimum Lumen Area Cut-Off Value in the Assessment of Intermediate Left Main Coronary Artery Lesions) showed that LM stenosis could be safely deferred with the guidance of IVUS.[22]It would be better if the physicians could get both IVUS and FFR information.However,it is hardly performed in clinical practice and also uneconomical for the patients.[23]According to a recent systematic review,deferring LM intermediate stenosis on the basis of FFR or IVUS showed an acceptable and similar risk of events in a mid-term follow-up.[24]
The recently developed UFR has the advantage of assessing detailed morphological measurement as well as functional ischemia information at the same time.As demonstrated before,compared with angiography-based FFR,the UFR calculating hyperemic flow relies on the reference lumen.By quantifying side branch ostia and delineation of the EEL contour from IVUS images,UFR reconstruct the reference lumen and thereafter the flow estimation.[13]Thus,UFR is more suitable for patients with complex coronary anatomy,LM or complex bifurcation stenosis,with vessel overlapping or significant foreshortening that angiography-based FFR might be difficult to obtain.
Concordance Among FFR,UFR and IVUS
It has been demonstrated that lesion located in LM was a predictor of worse concordance between FFR and instantaneous wave-free ratio.[25]In the present study,correlation between FFR and UFR was acceptable (r=0.67,with area under the curve by receiver operating characteristic of 0.94).Compared with regulator population (r=0.87),[13]the correlation between FFR and UFR among intermediate LM population was slightly lower.We observed a similar concordance between FFR and UFR in both lower MLA and higher MLA group with the cutoff value of 4.5 mm2or 6.0 mm2.
In our study,the cutoff value for MLA with 6.0 mm2showed better diagnostic performance as compared with the 4.5 mm2,which was similar with previously findings.The LITRO study showed LM stenosis with MLA large than 6.0 mm2is safely to be deferred.[22]El Hajj,et al.[26]described a good correlation between an 0.89 instantaneous wave-free ratio cutoff and 6.0 mm2IVUS.Rodriguez-Leor,et al.[25]also found that an MLA cutoff of 6.0 mm2best predicted an FFR > 0.80 and an iFR > 0.89.However,according to Park,et al,[27]a cutoff of 4.5 mm2for MLA was more suitable for Asiatic population.The present data showed that only 46% patients with FFR+had MLA≤ 4.5 mm2,while over 83% patients with FFR-had MLA > 4.5 mm2.Meantime,around 85% patients with FFR+had MLA ≤ 6.0 mm2;while over 30% of patients with FFR-had MLA > 6.0 mm2.The results showed higher specificity but lower sensitivity when using cutoff value of 4.5 mm2,while higher sensitivity but lower specificity when using cutoff value of 6.0 mm2.Thus,the optimal cutoff value of MLA used for strategy recommendation still need further study.
Safely Defer Treatment of Intermediate LM Lesion
When considering the possible serious adverse event caused by plaque rupture or erosion with thrombosis in LM location,physicians tend to believe“better safe than sorry”,setting a low threshold to perform invasive revascularization for intermediate LM stenoses.[28]In order to adequately manage those lesions,from guidelines to expert consensus,functional assessment was highly recommended.Although several types of wire derived pressure ratios were introduced,the utilization of pressure wirebased physiological assessment is limited in clinical practice.Not only for the risk of potential complications and higher costs,but the limited for the information of the plaque.Under this circumstance,UFR showed the advantage of providing both functional information and plaque details at the same time.On the other hand,UFR also showed advantages comparing with angiography-derived FFR in evaluating LM lesion due to notoriously inaccurate for estimating LM stenosis severity by angiography.According to the present study,UFR was proved to be a reliable tool to for functional evaluation of intermediate LM stenosis.
Study Limitations
The present study has several limitations.First,the present study is designed prospectively but without powered statistically assumption,therefore our findings did not allow for a conclusive interpretation and should be regarded as hypothesis-generating.Second,the analyzed population were relatively small and underpowered for primary endpoint.The small sample size results in a wider confidence interval for the area under the receiver-operating curves,diagnostic accuracy,sensitivity,and specificity.Third,most patients were identified with functional significant LM lesions (over 70%),which was slightly higher than previous report of intermediate LM population.Fourth,the estimated of intermediated LM stenosis was considered by the operator only.Nevertheless,the study presents patients in routine clinical practice.Fifth,the optimal cutoffs for MLA used in the present study were based on previous studies.Different thresholds for MLA,might results in different area under the curve and different comparison versus UFR.Finally,the present study didn’t evaluate clinical outcome by using a UFR-guided strategy.Future large-scale studies and randomized trials are warrant to demonstrate the diagnostic performance as well as prognostic value of the UFR in LM population.
Conclusions
In conclusion,UFR showed higher accuracy and good agreement with FFR as standard reference.The novel computational functional tool with both plaque details and physiology information was given great expectations to applied in the catheterization laboratory especially for complex coronary lesion including LM diseases.
DISCLOSURE
Fundings
This study was supported by CAMS Innovation Fund for Medical Sciences (CIFMS) (2022-12M-C&TB-043).
Conflict of Interest
None.
 Journal of Geriatric Cardiology2024年1期
Journal of Geriatric Cardiology2024年1期
- Journal of Geriatric Cardiology的其它文章
- Relationship between mitochondrial respiratory dysfunction of blood mononuclear cells and heart failure severity
- Multimorbidity and mortality among older patients with coronary heart disease in Shenzhen,China
- Effect of cytochrome P450 2C19 (CYP2C19) gene polymorphism and clopidogrel reactivity on long term prognosis of patients with coronary heart disease after PCI
- Influencing Factors on Cardiovascular Health in China
- Development and validation of a model integrating clinical and coronary lesion-based functional assessment for longterm risk prediction in PCI patients
- Interaction between systemic iron parameters and left ventricular structure and function in the preserved ejection fraction population: a two-sample bidirectional Mendelian randomization study