
Tissue engineering for urinary tract reconstruction and repair:Progress and prospect in China
2018-04-19 05:38QingsongZouQiangFu
Asian Journal of Urology 2018年2期
Qingsong Zou,Qiang Fu*
Department of Urology,Affiliated Sixth People’s Hospital,Shanghai Jiao Tong University,Shanghai,China
1.Introduction
Repair and reconstruction of urinary tracts are major issues in urology.A variety of techniques,such as resection of lesion,reconstruction with autologous tissue,and replacement with allografts,are used to manage these cases[1,2].Resection of lesions is not a practical option when extensive lesions exist,and it has lower success rates when compared with other procedures.However,the application of autologous transplantation is limited by donor site availability.Simultaneously,longer grafts induce higher donor site morbidity such as pain,swelling,post-operative infection,hemorrhaging,and even deformity[3,4].Additionally,donor organ shortage and tissue rejection block allogeneic transplantation in practical applications[2].Therefore,researchers increasingly focused on tissue engineering to repair urinary tract defects.Advances in tissue engineering can overcome the drawbacks of traditional therapeutic strategies and provide an alternative approach for urinary tract reconstruction and repair.Tissue engineering is a component of regenerative medicine that can remedy severe defects and restore normal functioning of tissues[5].In the last decade,numerous strategies for urinary tract regeneration were proposed in the field of tissue engineering.This study involved a review of cell sources,materials in urinary tract tissue engineering,and implantation techniques in China.The study also discusses the challenges and prospects of urinary tract tissue engineering.
2.Cell sources
A controversy is associated with the necessity of cell seeding in tissue-engineered urinary tracts.Most studies demonstrated that cell-free scaffolds could result in fibrosis post-operatively[6,7].With respect to extensive lesions,cell seeding is proposed to prevent scar formation[8]and improve tissue regeneration[9,10].A potential mechanism involves the promotion of rapid formation of urothelial barriers by cell-seeded scaffolds,and this can prevent urinary irritation.Urine is toxic to progenitor or stem cells recruited from normal adjacent tissues.Additionally,urine is also a major factor ofinflammatory infiltration that results in fibrous tissue deposition.Cell sources used in urinary tract reconstruction include differentiated primary cells and stem cells(Fig.1).
Autologous urothelial cells(UCs)are obtained from a urinary bladder that is commonly used in urinary tract reconstruction.A bladder biopsy is a commonly used method for harvesting bladder urothelial cells.A study by Romagnoli et al.[11]repaired posterior hypospadias with urethral epithelium harvested from a biopsy of urethral mucosa.However,these protocols are invasive due to surgical intervention and trauma to the bladder and urethra.A few researchers obtained urothelial cells from bladder washes and urine.The cells isolated from urine present the characteristics of normal bladder cells and are potentially promising for urethral reconstruction[12-14].Epidermal cells can be readily obtained from foreskin with only minor donor morbidity.These cells can be easily incubated and are sufficient in quantity when they are seeded on acellular matrix[15].Epithelial cells obtained from autologous oral are also adaptable for urinary tract substitution since their structure is similar to that of urothelium[16].Buccal mucosapossesses non-keratinizedastratifiedsquamous epithelium,which is highly resilient when exposed to greater mechanical abrasion.Oral keratinocytes are obtained by mechanically isolating the epidermis,and a traditional feeder dependent approachcanfacilitate expansion of oral keratinocytes.A biopsy can also induce donor morbidity.However,this approach is less invasive when compared with other epithelial cell sources from the urethra and bladder[17].Smooth muscle cells(SMCs)can be isolated from the bladder,and these cells increase the elasticity of caliber and prevent wall adhesions and collapsing via rapid formation muscle layer[18].Furthermore,transforming growth factor-β1(TGF-β1)secreted by SMCs can promote angiogenesis[19].Fibroblasts obtained from dermal tissue can secrete a series of cytokines and collagen that increase mechanical properties of the grafts and promote keratinocyte expansion[20].In renal tissue engineering,the presence of proximal tubule cells(PTCs)is crucial in maintaining kidney functioning and PTCs can be harvested from normal or diseased kidney tissues[21].PrimaryPTCcultures aremorerepresentativethan immortalized cell lines.However,primary kidney cells lose certain expressions ofimportant genes during passaging and possess limited proliferation potential[22].
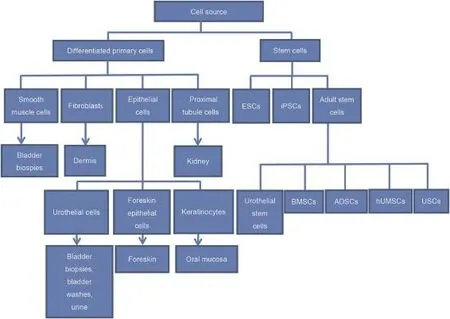
Figure 1 Cell sources in urinary tract reconstruction.ESCs,embryonic stem cells;iPSCs,induced pluripotent stem cells;BMSCs,bone marrow stem cells;ADSCs,adipose tissue-derived stem cells;hUMSCs,human umbilical cord-derived mesenchymal stem cells;USCs,urine-derived stem cells.
Stem cells are considered as undifferentiated cells and can differentiate into a wide variety of differentiated cells[23].Embryonic stem cells(ESCs)are theoretically considered as an ideal source of seeded cells due to multiple differentiation potential.However,the application is restricted by a major concern,namely the origin of their embryos and the probability of tumor formation[24].Additionally,ESCs can differentiate into urothelial cells when treated with alltrans retinoic acidin vitro[25].The ability to induce ESCs into urotheliumin vitroholds significant implications for urinary tract reconstruction[26].A controversy with respect to the application of ESCs exists.However,differentiation control is required prior to their use in regenerative medicine.Induced pluripotent stem cells(iPSCs)are an alternative to ESCs and possess important features similar to ESCs,such as proliferation and cloning capacities.Specifically,iPSCs can be generated from autologous adult somatic cells through a viral vectors approach to express the key factors SOX2,c-Myc,OCT4,and Klf4[27].Osborn et al.[26]developed an efficientin vitroinduction protocolforthe induction ofiPSCs into the urothelium to provide a novel source of bioengineered urothelium.
Adult stem cells(ASCs)from the tissues and organs of an adult,such as bone marrow,skin,and fat,constitute resident stem cells.These cells maintain homeostasis and regeneration of tissues after a minor injury due to proliferation and differentiation abilities[28].Additionally,ASCs are autologous and do not cause evident immune rejection.Moreover,these cells bypass ethical obstacles and are relatively easy to isolate.Urothelial stem cells,isolated from the ureter,urethra,and bladder possess a self-renewal feature and can differentiate into urothelium.A few reports demonstrated that urothelial stem cells in mice express sonic-hedgehog and p63 proteins[29,30].A study by Larsson et al.[31]isolated human urothelial cells and demonstrated that these cells possess the characteristics of clonogenicity,self-renewal,andmorphological differentiation.Bone marrow stem cells are obtained from bone marrow to generate SMCs and UCs[32,33].Nevertheless,a major concern relates to a small amount of stem cells in bone marrow that entails significant time to expandin vitroto obtain adequate cells.Additionally,the process ofisolating can lead to discomfort because of bone marrow aspiration.Adipose tissue-derived stem cells(ADSCs)are similar to mesenchymal stem cells from bone marrow stroma with a stableundifferentiatedandhighproliferativestatusin vitro.They can differentiate into multiple cell lineage including SMC and UC[34].The coculturing of ADSCs with UCs or treated with all-trans retinoic acid leads to the differentiation of ADSCs into UCs[35,36].Specifically,in a previous study,ADSCs maintained their phenotype for 2 weeksin vitroprior to implantation in nude mice[37].These findings suggested that ADSCs can be an ideal source for urinary tract reconstruction due to a minimally invasive procedure and the presence of abundant quantities in adipose tissue[38].Human umbilical cord-derived mesenchymal stem cells(hUMSCs)are obtained from fresh cord blood and may be an excellent source of ASCs due to their multipotent differentiation ability[39,40].Importantly,hUMSCs transplants exhibit less immunologic rejection when compared to other ASCs,and this property makes them ideal candidates for urinary tract repair and reconstruction[41].Urine-derived stem cells(USCs)can be isolated from urine and do not involve a risk of teratoma formation.Furthermore,USCs possess significant proliferative capacity and can produce a considerable number of cells from a small amount of cells[42,43].The treatment of USCs with appropriate media leads to their differentiation into multiple cell types including UCs and SMCs that constitute major seeded cells in urinary tract reconstruction[44].
3.Biomaterials
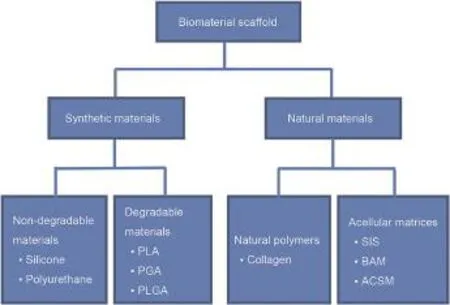
Figure 2 Biomaterials in urinary tract reconstruction.PLA,polylactic acid; PGA, polyglycolic acid; PLGA, polylacticcoglycolic acid;SIS,small intestinal submucosa;BAM,bladder acellular matrices;ACSM,acellular corpus spongiosum matrices.
Biomaterials control the biological microenvironment and provide a three-dimensional(3D)space for regenerated tissues[45].The functions of scaffolds used in tissue engineering are dependent on the properties of selected biomaterials[46].Thus,in addition to the role of delivery vehicles to transport nutrients and wastes[47],the properties of the selected biomaterials must also include the functions of promoting proliferation,differentiation,and attachment[48].Ideal biomaterials should possess a controlled degradation rate without toxicity.A variety of biomaterial scaffolds were used for urinary tract reconstruction.These are classified into two major types,namely synthetic and natural biomaterials(Fig.2).The first type includes non-degradable materials(such as silicone and polyurethane)and biodegradable polymers such as polylactic acid(PLA),polyglycolic acid,and polylacticcoglycolic acid(PLGA).Non-degradable materials used in urinary tract reconstruction exhibited poor results with the occurrence of a variety of complications such as calcification and fistulae[49].In contrast,biodegradable scaffolds are mostly used in urinary tract reconstruction as they exhibit better results[50].Natural materials include the following two groups:natural polymers(mostly collagen)and acellular matrices obtained from cadaveric or animal organs via enzymatic,physical,or chemical methods[51].A study by Nuininga et al.[52]repaired urethral lesions with cross-linked collagen and compressed collagen structures in rabbit models,and retrograde urethrography showed a normal caliber at 2 weeks postsurgery.The most commonly used acellular tissue matrices in urethral reconstruction are small intestinal submucosa(SIS),bladder acellular matrices(BAM),and acellular corpus spongiosum matrices.It is necessary to choose between synthetic and naturalscaffolds prior to the use of a scaffold in urinary tract reconstruction.Synthetic scaffolds are advantageous as they are easily available,highly reproducible,and possess excellent mechanical properties.However,synthetic scaffolds involve the absence of cytokines and extracellular matrix(ECM)proteins that are major factors in regulating cellular proliferation and differentiation and mimic the microenvironment[53].Afewsynthetic polymers canresult in inflammatory responsesin vivoand generate acidic products that impaircellular growth[54].Naturalscaffolds reserve 3D structure and bioactive factors of the original tissue and represent biocompatible and biodegradable materials[55].However,naturalscaffolds are characterized by the absence of structural strength and biochemical properties that are dif ficult to control.These properties are associated with fibrosis and contracture when implanted into urethra[56].
4.Tissue engineering approaches for renal repair and reconstruction
The kidney is an important organ with multiple functions such as filtration function,erythropoietin secretion,and regulation of electrolytes and pH.The filtration function is the most important function among these functions.The filtration function is mainly dependent on a nephron that is composed of various types of cells and complicated vascular structures.Additionally,it is also necessary to consider other functions when researchers construct fully functional kidneys.Tissue engineering approaches for renal repair and reconstruction as reported in China are listed in Table 1.
Renal function can be ameliorated via cell-only approaches in renal regeneration.Pluripotent stem cells(PSCs)can differentiate into different cell types and form heterogeneous tissues due to the self-assembling approach[57,58].Specifically,PSCs are composed of ESCs and iPSCs that may provide alternative cell types for kidney regeneration.International studies reported that PSCs can generateintermediatemesodermandmetanephric mesenchyme cells that constitute nephron progenitor cells[59].Despite these advances,this approach has not succeeded in constructing multi-function kidneys due to the absence of other functions in the regenerated kidneys.
The mesenchymal stem cells(MSCs)play a vital role in preserving renal parenchymal integrity from acute damage.Possible mechanisms of MSCs include the promotion of tubular epithelium regeneration,secretory functions,and peri-tubular capillary regeneration.Chen et al.[60]used ADSC to repair renal function following acute ischemia-reperfusion injury.The results indicated that ADSC could minimize kidney damage through the suppression ofinflammatory response and promotion of angiogenesis.Furthermore,MSCs derived from human umbilical cord(UCMSCs)possess stem cell properties and represent a more abundant and safer source for stem cell therapy.Cao et al.[61]demonstrated that UC-MSCs can ameliorate renal functions inischemia/reperfusion-inducedacuterenal failure via replacement ofinjured tissues and secretion relative cytokines.Growth factors,such as vascular endothelial growth factor(VEGF),epidermal growth factor,and hepatocyte growth factor(HGF),can increase the therapeutic effect in the therapy of acute kidney injury(AKI)[62].Yuan et al.[63]utilized human embryonic MSC combined with VEGF to heal cisplatin-injured renal failure.Chen et al.[64]reported a similar study to evaluate the effect of HGF modified human umbilical cord-derived mesenchymal stem cells on AKI,and the results further confirmed the vital role of growth factors on stem cell therapy.Exosomes are microvesicles released from various cells and are present in extracellular space.Exosomes include a number of components such as mRNA,microRNA and proteins.Previous studies demonstrated that hUMSC-excretedexosomes reducecisplatin-inducedoxidative stress by decreasing the formation of products and promoting cell proliferation[65].
The kidney is an organ with a complex structure and functions,and it is composed of multiple cell types and acomplicated vascular network.Guan et al.[66]introduced a decellularization technology to produce kidney acellular matrices from porcine that retained the 3D architecture and the vascular tree.Further studies were not performed to recellularize the scaffold with autologous cells.However,this study could have important implications for kidney regeneration since the size and architecture ofthe kidneysin the studies was similar to those of human kidneys.Yu et al.[67]produced a decellularized kidney scaffold from rats and implanted the same into a kidney afterpartialnephrectomy.Renalfunctionswere restored atsix weekspost-implantation because of physical support as well as biochemical cues of the kidney scaffold.However,the cell-free scaffolds are not feasible in creating transplantable kidneys due to the absence of residual cells.Studies investigate the use of scaffolds combined with stem cells to generate a whole kidney.Guan et al.[68]utilized decellularized kidney scaffolds from rats and mice ESCs to recellularize kidney scaffolds.The fore-mentioned scaffolds were orthotopically implanted in rats,and the structure and major functions exhibited by the recellularized kidney were similar to those of native kidneys.This approach indicated that it is possible to reconstruct transplantable kidneys free from immune response.
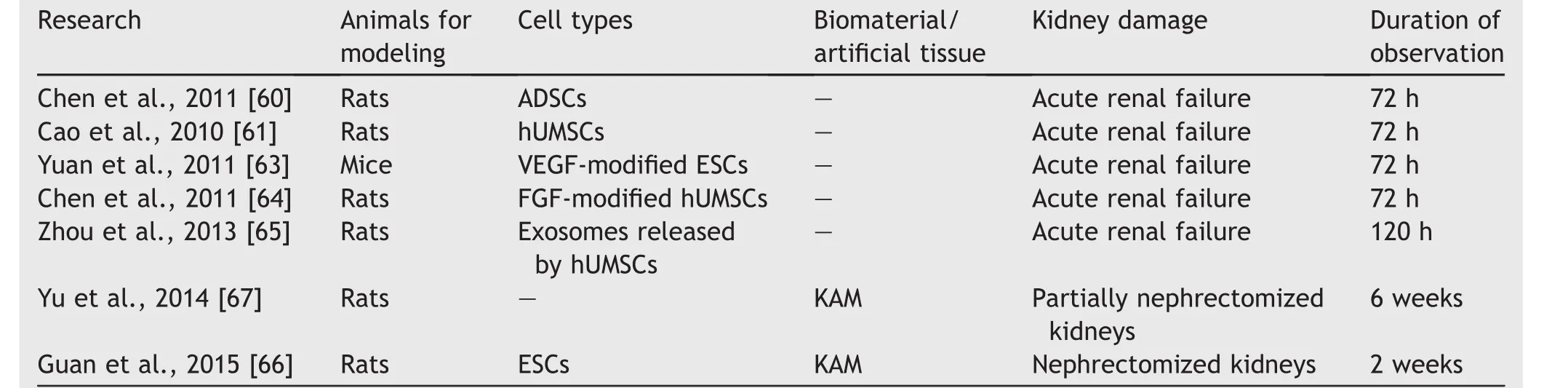
Table 1 Tissue engineering approaches used for renal reconstruction in China.
5.Tissue engineering approaches for ureteral reconstruction
Research focused on ureteral tissue engineering is limited when compared with that focused on other organs in the urinary system.Table 2 shows tissue engineering approaches for ureteral reconstruction as reported in China.Most international studies used bare scaffolds in ureteral tissue engineering and demonstrated poor results due to fibrosis and in flammation,which indicated the necessity of cell-seeding[69,70].Two crucial cell types in the ureter include the following:human UCs that form a permeability barrier to prevent the reabsorption of toxic urine,and SMCs that are responsible for contractile function and compliance of the ureter through smooth muscle layers.Several researchers chose autogenous UCs as seeded cells to prevent chronic immune response and fibrosis[71-73].The main difference in the three fore-mentioned studies involves the method used to obtain ideal biomaterials with mechanical properties,biocompatibility,and low toxicity.Fu et al.[71]and Xu et al.[72]utilized poly-L-lactic acid(PLLA)combinedwithcollagenanddecellularized matrices,respectively,to achieve composited scaffolds.These composited scaffolds provide a favorable surface for cell proliferation and attachment and possess good mechanical properties.Another study transplanted PLLA stents into subcutaneous tissues of rats to form connective tissue capsules on surfaces and these connective tissue capsules were decellularized and further recellularized[73].However,the disadvantage of autogenous cells in ureteral tissue engineering is that biopsies do not harvest sufficient cells especially in patients with urologic cancer or extensive tissue damage.Under these types of conditions,stem cells can constitute the ideal origin for ureteral tissue engineering.Liao et al.[9]seeded MSCs and SMCs onto bladder acellular matrices(BAM),and the cell-seeded grafts were transplanted into the omentum of a rabbit prior toureteral reconstruction.Furthermore,ADSCs possess the potential to differentiate into epithelial cells and SMCs.Moreover,ADSCs are already used to differentiate SMCs in tissue engineering urethra[10].Additionally,Shi et al.[37]differentiated ADSCs into urothelial lineage and then seeded the same on PLA/collagen scaffolds.A similar study constructed a tissue-engineered ureteral by seeding ADSCs and SMCs on bladder submucosa matrix(BSM).Multilayered urothelium and neovascularization are observed in the graft[74].
6.Tissue engineering approaches for bladder reconstruction
A variety of studies on bladder reconstruction were reported in China(Table 3).The cell-free scaffolds approach can be an ideal strategy for bladder reconstruction because this strategy is simple and does not require cell harvesting and culturein vitro.With respect to the scaffolds,BAM and SIS are widely used in bladder reconstruction.Zhu et al.[75]and Wang and Liao[76]evaluated the potential use of BMA and SIS,respectively,as bioscaffolds in tissue engineering bladder in the rabbit model.The results of both studies showed that regenerated bladders possessed similar histologic and functional properties.Zhao et al.[77]produced a bilayer scaffold using a silk fibroin combinedbladder acellular matrix and proved that these biomaterials promote vessel and nerve regeneration.However,the cellfree scaffolds approach is unsuitable for larger bladder regeneration.An increase in bladder defects leads to a significant decrease in the ability of a vascular network to supply sufficient nutrients for the cells,and the remaining bladder provides insufficient structural support.In order to overcome these limitations,increasing attention is focused on a method of promoting smooth muscle regeneration and neovascularization.As is widely known,growth factors play vital roles in the bladder development and regeneration.Although a natural ECM retains bioactive factors,the amount of factors is insufficient for bladder regeneration.Specifically,VEGfis a crucial bioactive factor that regulates an adjacent endothelial cell to migrate and proliferatein situand promote vasculature formation.Bioscaffolds combined with VEGF to promote neovascularization are widely used in bladder regeneration[78,79].Furthermore,FGF and platelet-derived growth factor-BB(PDGF-BB)are used to promote smooth muscle regeneration and accelerate neovascularization of a bladder[80-82].A few researchers incorporated bioscaffolds with multiple growth factors,and the results revealed that multiple growth factors exhibited a significantly favorable performance in neovascularization and inhibition of contracture when compared with a single growth factor[82,83].
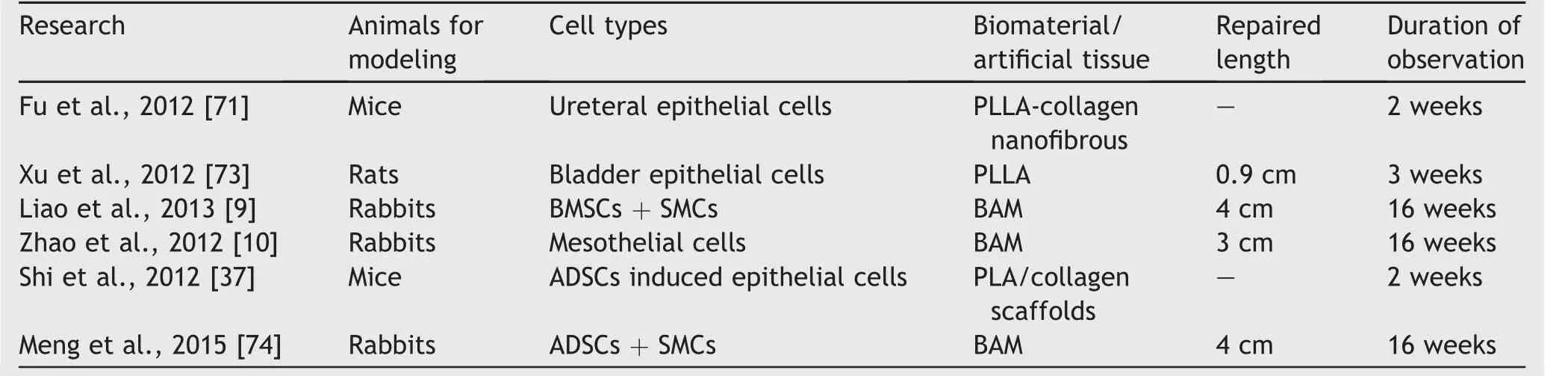
Table 2 Tissue engineering approaches for ureteral reconstruction in China.
Cell-seeded technology on biomaterials and synthetic polymers are introduced to avoid immunological rejection and improve the regeneration process.Autologous endothelial cells can act as an alternative to rapidly establish blood supply in addition to the strategy ofincorporating growth factors into biomaterials.However,endothelial progenitor cells are more desirable than endothelial cells because of their less invasive harvesting procedure[84,85].Additionally,UC and SMC are crucial cells in the generation of an ideal bladder due to their roles in urinary barrier and mechanical support.Internationally,studies demonstrated that biomaterials seeded with both cells can generate an organized bladder albeit not in cell-free biomaterials[86].This approach is not suitable for patients with bladder cancer despite advances in seeding materials with UC and SMC.Therefore,increasing attention is focused on stem cells as alternative cell sources for bladder reconstruction.ASCs harvested from bone marrow or adipose or umbilical cord tissues can overcome these limitations.However,the use of MSCs is not always acceptable because of an invasive harvesting process and limited cells.Zhu et al.[87]and Zhe et al.[88]assessed the feasibility of ADSC seeded on BAM for bladder reconstruction.The results demonstrated that the approach could promote the regeneration of nervous tissues and smooth muscles in a rabbit model.Another ideal source of cell transplantation involves hUMSC isolated from human umbilical cord tissues.These cells present minimal rejection and do not involve any ethical controversy.Yuan et al.[89]selected hUMSC-seeded BAMs to reconstruct a bladder.The results showed the presence of complete layers of urothelium and smooth muscles.
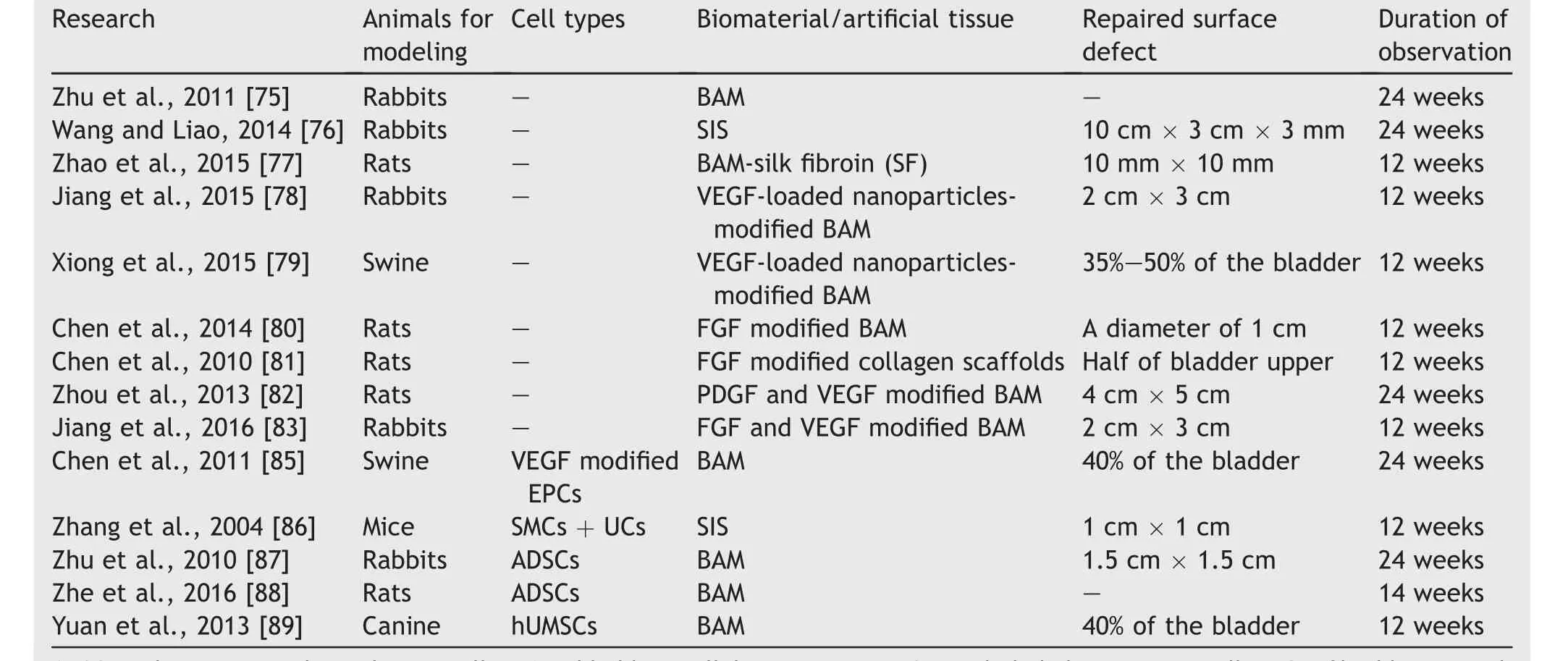
Table 3 Tissue engineering approaches for bladder reconstruction in China.
7.Tissue engineering approaches for urethral reconstruction
Tissue engineering for urethral reconstruction mainly includes the following two approaches:cell-free grafts and cell-seeded grafts.Cell-free matrices are considered as an“off the shelf” material due to the ease of production.Additionally,the morbidity of a donor may be reduced,since no surgical procedures are required for cell harvesting.Table 4 lists the cell-free graft approaches applied in urethral reconstruction in China.
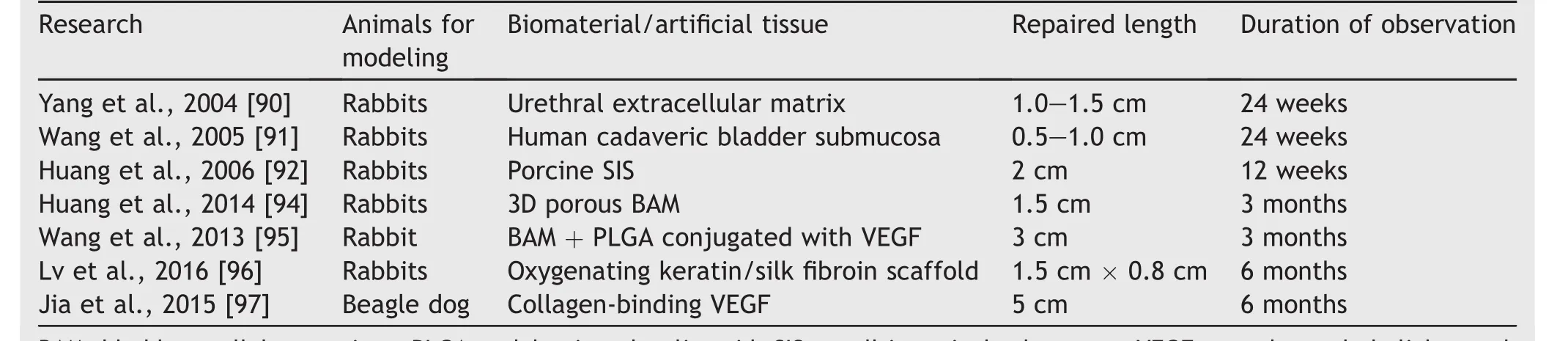
Table 4 Cell-free grafts applied in urethral reconstruction in China.
Yang et al.[90]used a urethral ECM from rabbit urethral tissue to repair urethral segmental defects(with a length of 2 cm)in male rabbits.Wang et al.[91]and Huang et al.[92]conducted the similar studies using BAM and SIS to repair urethral segmental defectsinrabbits,respectively.Although satisfactory results were obtained in the forementioned studies,the length of the urethra defect is shorter(<2 cm),and the matrices used in urethral reconstruction corresponded to patch grafts and not tubular grafts.Acellular matrices repair urethra by guiding the regeneration of urothelial cells and connective tissue.Thus,an acellular graft may be feasible only when the urethral wall is healthy and rich in blood.A few scaffold parameters,such as porosity,can influence the transport of waste products and nutrients.Appropriate pore size promotes proliferation,infiltration,and differentiation of cells[93].Huang et al.[94]used BAM treated with peracetic acid(PAA)to form three dimensional structural constructs to repair urethral defects.Their results revealed that PAA-treated BAM promoted the regeneration of urothelium and neovascularization when compared with the non-PAA-treated BAM group.Additionally,VEGfis an important cytokine that promotes angiogenesis,and it plays a major role in urethral reconstruction.Wang et al.[95]suggested BAM stents modified by PLGA with sustained-release of VEGF may serve as a matrix substitute to repair anterior urethral stricture(with a length of 3 cm)in rabbits.In addition to the angiogenesis effect,VEGF also reduces collagen deposition and minimizes scar formation in engineering urethral reconstruction.Lv et al.[96]incorporated an oxygen-generating substance into keratin/silk fibroin to construct oxygen-generative synthetic materials.An evaluation indicated that the oxygen-generative scaffold promoted the regeneration of urinary tract defects and decreased inflammatory response after implantation.The prevalent view is that cell-free biomaterials are feasible in short strictures.Unseeded biomaterials are less successful when the length of urethral strictures exceeds 4 cm[3].However,Jia et al.[97]utilized collagen scaffolds modified with VEGF to repair extensive urethral defects(with a length of 5 cm)in a beagle dog.Although,biomaterials modified with VEGF may provide a novel strategy for longer urethral reconstruction,it is necessary to conduct further studies to prove the feasibility of this strategy.
To summarize,the applications of cell-free biomaterials in the treatment of urethral strictures are limited.An international consensus is that cell-free biomaterials are only feasible in short strictures when a healthy and wellvascularized part of a urethral wall exists[98].The limitations of the cell-free grafts prompted researchers to search for other suitable approaches.Autologous cell seeded grafts were proposed to overcome the deficiencies observed with acellular grafts.Multiple studies using cellseeded grafts in urethral reconstruction are reported in China as listed in Table 5.
Fu et al.[15,99]expanded epidermal cells acquired from autologous foreskin and seeded onto allogeneic rabbit bladder submucosa to reconstruct anterior urethra.The source of epidermal cells is abundant,and the approach ofisolating cells is less invasive.Xie et al.[100]selected electrospun silk fibroin matrices as a material and combined it with urothelial cells from bladder biopsies to repair a urethra.This scaffold exhibited 3D properties and porosity,and the poor mechanical properties were improved by postprocessing the material.Autologous mesothelial cells isolated from omentum biopsies can be used for tubularized urethral reconstruction.Gu et al.[101]used BAM and mesothelial cells to construct tissue-engineered urethra in a rabbit model.
Furthermore,ADSCs are abundant in quantity and less invasive to a donor site when compared with other cell sources and can differentiate into epithelial cells with the stimulation of factors[102].Li et al.[38]utilized rabbit adipose-derived stem cells to differentiate epithelium(Epith-rADSCs)and seeded epithelium into BAM to repair urethra defects.Amniotic membrane(AM),which is a urethral substitution with less inflammation and a lower risk of rejection,exhibits significant potential in urethral reconstruction[103].Wang et al.[104]selected the cell-seeded denuded human amniotic scaffold(dHAS)as urethral reconstruction materials in rabbit models.The evaluation indicated good results in which urethral defects were completely resolved and a mild inflammatory response was observed.Li et al.[105]proposed the reconstruction of tissue-engineered urethra with marrow MSCs and SMCs.Marrow MSCs and SMCs were isolated and constructed into cell sheets prior to seeding into BAM.
It is widely accepted that TGF-β1 may result in scar formation.Li et al.[106]built tissue-engineered urethra with oral keratinocyte and fibroblasts transfected TGF-β1 siRNA.A wide caliber without fibrosis and inflammation was observed after 6 months.Although this approach can significantly inhibit fibrosis because of the reduction in ECM production,genetic technology limited the application in clinics due to technical aspects.It was demonstrated that TGF-β could promote ECM secretion by regulating the Wnt signaling pathway.Zhang et al.[107]incorporated a Wnt pathway inhibitor(ICG-001)and collagen/poly(L-lactideco-caprolactone)viaanelectrospinningtechniqueto construct a scaffold for urethroplasty.A stable oxygen supply is the key point to maintain the survival and cell viability of seeded cells.Huang et al.[108]used a gelatin sponge to create a porous structure for bacterial cellulose scaffolds and selected lingual keratinocytes as seeded cells to repair urethral defects(with a length of 2 cm)in rabbits.The 3D porous structure is conducive to cell infiltration and vascularization,and thus the epithelium layer density and smooth muscle and vessel density were higher.different from actual clinical urinary tract injuries,and this could account for better results achieved in experimental studies.Furthermore,most researchers in China conducted experiments by using rabbits or rats as opposed to large animals.The urine of rabbits contains high levels of calcium that can penetrate into the collagen due to the strong adsorption capacity[49].Atala et al.[109]also proposed that large animals can better mimic the conditions prevalent in humans.Although,a large amount of research focused on urinary tract reconstruction was reported in China,clinical studies that limit the application of tissue engineering urethra were not performed.Additionally,a selected ideal cell should be easy to isolate and sufficient in quantity for expansionin vitro.Stem cells possess a multiple differentiation potential.Thus,specific environments should be provided for stem cells recruitment and differ-
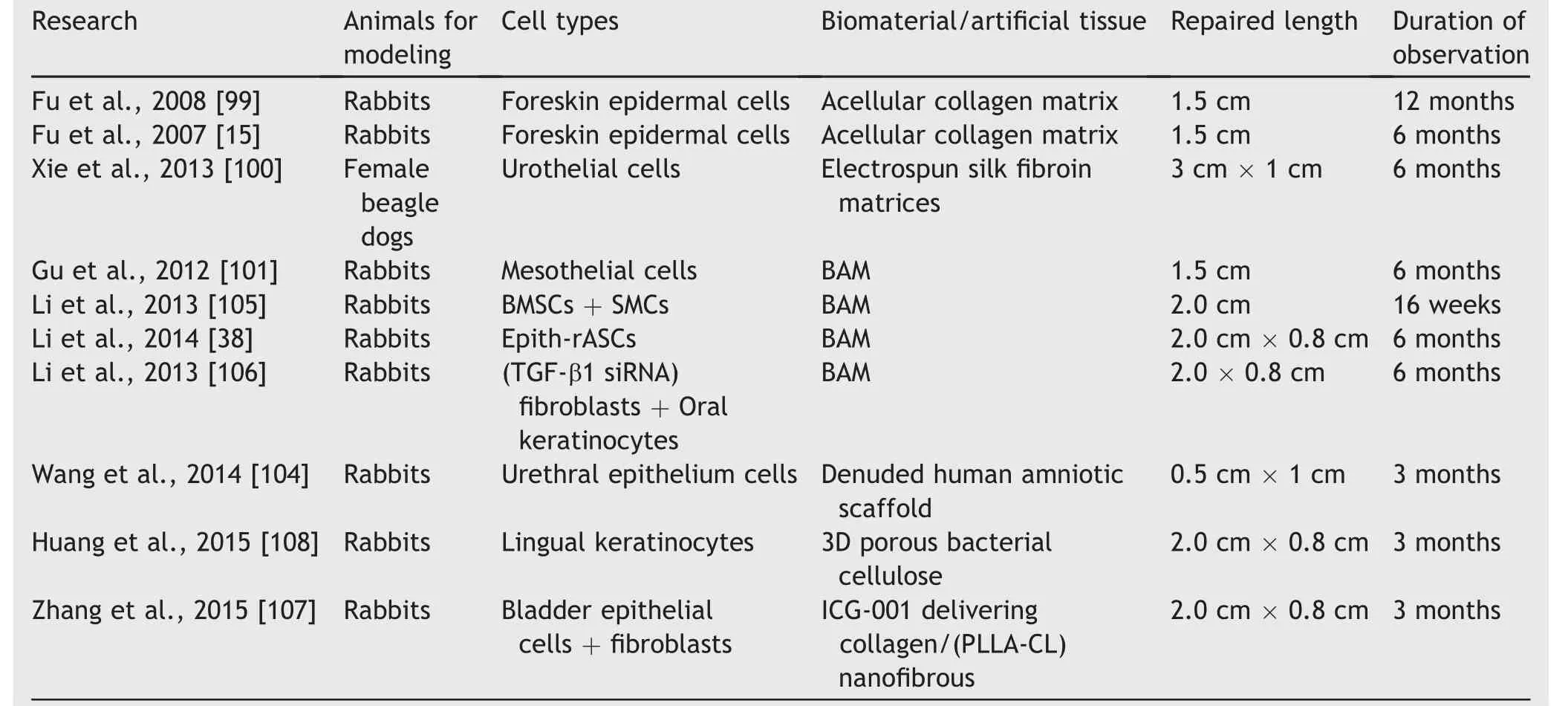
Table 5 Cell-seeded grafts applied in urethral reconstruction in China.
A cell-seeded graft includes disadvantages such as requiring a period of cell culture in a clean room laboratory.Thus,it is presently not suitable as an “off the shelf”product.There are also cost and time implications.The cost of a cellularized graft is six times that of a noncellularized graft[3].It is necessary to perform further studies to reduce the cost-effectiveness of this approach.
8.Current challenges and future directions
Although there is significant progress in urinary tract tissue engineering,it is necessary to resolve certain problems.The creation of an ideal animal model for urinary tract reconstruction is a problem.Most studies created a defect intra-operatively andimmediately repairedthesame with substitution.However,defects in animal models are entiation to regulate migration and directional differentiation[110].
Idealscaffoldsshouldpossesscharacteristicsof biocompatibility,biodegradability,low toxicity,and excellent mechanical strength.It is also important to ensure a suitable microenvironment to promote cell adhesion and tissue organization.Generally,a few synthetic polymers possess excellent mechanical properties and are biodegradable.However,a poor microenvironment exists,and it is similar to the limited application of native tissues in urethral reconstruction.In contrast,naturally derived materials are biocompatible and biodegradable and maintain important bioactive factors.However,these materials possess poor mechanical properties.Fu et al.[71]fabricated composite scaffolds that are constructed synthetic materials combined with a natural matrix by using electrospinning technology.The composite scaffolds favor cell attachment and distribution due to excellent biocompatibility and mechanical strength.The electrospun composite scaffolds can be used as alternative cell carriers for urinary tract reconstruction.Theself-assemblymethodcan construct tissue autologous cells and produce a dense ECM.When compared with other exogenous scaffolds models,the self-assembly method possesses biocompatibility and lower inflammatory response that increases the success rate of urethral reconstruction[111].In this method,cells can receive differentiation signals in a manner similar to that of native tissues.Although this technique is time consuming,it may provide a promising approach to repair tract tissue defects.
Bioprinting technology has emerged as a new technology for constructing tissue and organs in tissue engineering.This technology enables the simultaneous printing of 3D cells and biomaterials in precise locations within 3D structures.Magnetic resonance imaging and CT scans are used to obtain 3D information related to a tissue or organ and guide specific types of cells and materials into precise locations to mimic the architecture of native tissue construction.Currently,bioprinting techniques can build a series of tissues such as aortic valves[112]and skeletal muscles[113].Hence,the bioprinting technique exhibits significant potential in tissue engineering and can offer a new approach for tract tissue reconstruction.
9.Conclusion
Although promising progress has been made in the tissue engineering for urinary tract reconstruction in China,these promising results are showed only in animal studies and several issues remain unresolved,such as the ideal cell source,biomaterials and animal models.In addition,further research with larger numbers of patients needs to be conducted to confirm the safety and feasibility of tissue engineering for urinary tract reconstruction.Still,we believe that tissue engineering approach will provide a huge benefit for patients with urinary tract depicts in the future.
Conflicts ofinterest
The authors declare no conflict ofinterest.
[1]Mangera A,Chapple C.Management of anterior urethral stricture:an evidence-based approach.Curr Opin Urol 2010;20:453-8.
[2]Badylak SF,Taylor D,Uygun K.Whole-organ tissue engineering:decellularization and recellularization of threedimensional matrix scaffolds.Annu Rev Biomed Eng 2011;13:27-53.
[3]Mangera A,Chapple CR.Tissue engineering in urethral reconstruction-an update.Asian J Androl 2013;15:89-92.
[4]Lumen N,Oosterlinck W,Hoebeke P.Urethral reconstruction using buccal mucosa or penile skin grafts:systematic review and meta-analysis.Urol Int 2012;89:387-94.
[5]Atala A.Recent applications of regenerative medicine to urologic structures and related tissues.Curr Opin Urol 2006;16:305-9.
[6]El-Assmy A,Hafez AT,El-Sherbiny MT,El-HamidMA,Mohsen T,Nour EM,et al.Use of single layer small intestinal submucosa for long segment ureteral replacement:a pilot study.J Urol 2004;171:1939-42.
[7]Liatsikos EN,Dinlenc CZ,Kapoor R,Bernardo NO,Pikhasov D,Anderson AE,et al.Ureteral reconstruction:small intestine submucosa for the management of strictures and defects of the upper third of the ureter.J Urol 2001;165:1719-23.
[8]Chen F,Yoo JJ,Atala A.Experimental and clinical experience using tissue regeneration for urethral reconstruction.World J Urol 2000;18:67-70.
[9]Liao W,Yang S,Song C,Li X,Li Y,Xiong Y.Construction of ureteral grafts by seeding bone marrow mesenchymal stem cells and smooth muscle cells into bladder acellular matrix.Transplant Proc 2013;45:730-4.
[10]Zhao Z,Yu H,Xiao F,Wang X,Yang S,Li S.Differentiation of adipose-derived stem cells promotes regeneration of smooth muscle for ureteral tissue engineering.J Surg Res 2012;178:55-62.
[11]Romagnoli G,De Luca M,Faranda F,Bandelloni R,Franzi AT,Cataliotti F,et al.Treatment of posterior hypospadias by the autologous graft of cultured urethral epithelium.N Engl J Med 1990;323:527-30.
[12]Zhang Y,McNeill E,Tian H,Soker S,Andersson KE,Yoo JJ,et al.Urine derived cells are a potential source for urological tissue reconstruction.J Urol 2008;180:2226-33.
[13]Nagele U,Maurer S,Feil G,Bock C,Krug J,Sievert KD,et al.In vitroinvestigations of tissue-engineered multilayered urothelium established from bladder washings.Eur Urol 2008;54:1414-22.
[14]Fossum M,Skikuniene J,Orrego A,Nordenskjold A.Prepubertal follow-up after hypospadias repair with autologousIn vitrocultured urothelial cells.Acta Paediatr(Oslo,Norway:1992)2012;101:755-60.
[15]Fu Q,Deng CL,Liu W,Cao YL.Urethral replacement using epidermal cell-seeded tubular acellular bladder collagen matrix.BJU Int 2007;99:1162-5.
[16]Bhargava S,Patterson JM,Inman RD,MacNeil S,Chapple CR.Tissue-engineered buccal mucosa urethroplasty-clinical outcomes.Eur Urol 2008;53:1263-9.
[17]Rheinwald JG,Green H.Serial cultivation of strains of human epidermal keratinocytes:the formation of keratinizing colonies from single cells.Cell 1975;6:331-43.
[18]Orabi H,AbouShwareb T,Zhang Y,Yoo JJ,Atala A.Cellseeded tubularized scaffolds for reconstruction of long urethral defects:a preclinical study.Eur Urol 2013;63:531-8.
[19]Zhu C,Ying D,Zhou D,Mi J,Zhang W,Chang Q,et al.Expression of TGF-beta1 in smooth muscle cells regulates endothelial progenitor cells migration and differentiation.J Surg Res 2005;125:151-6.
[20]Xie M,Xu Y,Song L,Wang J,Lv X,Zhang Y.Tissue-engineered buccal mucosa using silk fibroin matrices for urethral reconstruction in a canine model.J Surg Res 2014;188:1-7.
[21]Phillips AO,Steadman R.Diabetic nephropathy:the central role of renal proximal tubular cells in tubulointerstitial injury.Histol Histopathol 2002;17:247-52.
[22]Cummings BS,Lasker JM,Lash LH.Expression of glutathionedependent enzymes and cytochrome P450s in freshly isolated and primary cultures of proximal tubular cells from human kidney.J Pharmacol Exp Ther 2000;293:677-85.
[23]Blau HM,Brazelton TR,Weimann JM.The evolving concept of a stem cell:entity or function?Cell 2001;105:829-41.
[24]Fuchs E,Segre JA.Stem cells:a new lease on life.Cell 2000;100:143-55.
[25]Mauney JR,Ramachandran A,Yu RN,Daley GQ,Adam RM,Estrada CR.All-trans retinoic acid directs urothelial specification of murine embryonic stem cells via GATA4/6 signaling mechanisms.PLoS One 2010;5:e11513.
[26]Osborn SL,Thangappan R,Luria A,Lee JH,Nolta J,Kurzrock EA.Induction of human embryonic and induced pluripotent stem cells into urothelium.Stem Cells Transl Med 2014;3:610-9.
[27]Hart ML,Neumayer KM,Vaegler M,Daum L,Amend B,Sievert KD,et al.Cell-based therapy for the deficient urinary sphincter.Curr Urol Rep 2013;14:476-87.
[28]Ilic D,Polak JM.Stem cells in regenerative medicine:introduction.Br Med Bull 2011;98:117-26.
[29]Shin K,Lee J,Guo N,Kim J,Lim A,Qu L,et al.Hedgehog/Wnt feedback supports regenerative proliferation of epithelial stem cells in bladder.Nature 2011;472:110-4.
[30]Pignon JC,Grisanzio C,Geng Y,Song J,Shivdasani RA,Signoretti S.p63-expressing cells are the stem cells of developing prostate,bladder,and colorectal epithelia.Proc Natl Acad Sci U S A 2013;110:8105-10.
[31]Larsson HM,Gorostidi F,Hubbell JA,Barrandon Y,Frey P.Clonal,self-renewing and differentiating human and porcine urothelial cells,a novel stem cell population.PLoS One 2014;9:e90006.
[32]Tian H,Bharadwaj S,Liu Y,Ma PX,Atala A,Zhang Y.Differentiation of human bone marrow mesenchymal stem cells into bladder cells:potential for urological tissue engineering.Tissue Eng Part A 2010;16:1769-79.
[33]Sharma AK,Hota PV,Matoka DJ,Fuller NJ,Jandali D,Thaker H,et al.Urinary bladder smooth muscle regeneration utilizing bone marrow derived mesenchymal stem cell seeded elastomeric poly(1,8-octanediol-co-citrate)based thin films.Biomaterials 2010;31:6207-17.
[34]Orabi H,Lin G,Ferretti L,Lin CS,Lue TF.Scaffoldless tissue engineering of stem cell derived cavernous tissue for treatment of erectile function.J Sex Med 2012;9:1522-34.
[35]Brzoska M,Geiger H,Gauer S,Baer P.Epithelial differentiation of human adipose tissue-derived adult stem cells.Biochem Biophys Res Commun 2005;330:142-50.
[36]Liu J,Huang J,Lin T,Zhang C,Yin X.Cell-to-cell contact induces human adipose tissue-derived stromal cells to differentiate into urothelium-like cellsin vitro.Biochem Biophys Res Commun 2009;390:931-6.
[37]Shi JG,Fu WJ,Wang XX,Xu YD,Li G,Hong BF,et al.Tissue engineering of ureteral grafts by seeding urothelial differentiated hADSCs onto biodegradable ureteral scaffolds.J Biomed Mater Res Part A 2012;100:2612-22.
[38]Li H,Xu Y,Xie H,Li C,Song L,Feng C,et al.Epithelialdifferentiated adipose-derived stem cells seeded bladder acellular matrix grafts for urethral reconstruction:an animal model.Tissue Eng Part A 2014;20:774-84.
[39]Barachini S,Trombi L,Danti S,D’Alessandro D,Battolla B,Legitimo A,et al.Morpho-functional characterization of human mesenchymal stem cells from umbilical cord blood for potential uses in regenerative medicine.Stem Cells Dev 2009;18:293-305.
[40]Secco M,Zucconi E,Vieira NM,Fogaca LL,Cerqueira A,Carvalho MD,et al.Multipotent stem cells from umbilical cord:cord is richer than blood!Stem Cells(Dayton,Ohio)2008;26:146-50.
[41]Xu Y,Sun DC,Wei ZT,Hong BF,Yang Y.Experimental study on transplantation of autologous minced muscle with human umbilical cord mesenchymal stem cells for urethral reconstruction.Eur Rev MedPharmacol Sci 2014;18:3412-9.
[42]Bharadwaj S,Liu G,Shi Y,Wu R,Yang B,He T,et al.Multipotential differentiation of human urine-derived stem cells:potential for therapeutic applications in urology.Stem Cells(Dayton,Ohio)2013;31:1840-56.
[43]Bodin A,Bharadwaj S,Wu S,Gatenholm P,Atala A,Zhang Y.Tissue-engineered conduit using urine-derived stem cells seeded bacterial cellulose polymer in urinary reconstruction and diversion.Biomaterials 2010;31:8889-901.
[44]Zhang D,Wei G,Li P,Zhou X,Zhang Y.Urine-derived stem cells:a novel and versatile progenitor source for cell-based therapy and regenerative medicine.Genes Dis 2014;1:8-17.
[45]Davis ME,Hsieh PC,Grodzinsky AJ,Lee RT.Custom design of the cardiac microenvironment with biomaterials.Circ Res 2005;97:8-15.
[46]Hutmacher DW,Cool S.Concepts of scaffold-based tissue engineering-the rationale to use solid free-form fabrication techniques.J Cell Mol Med 2007;11:654-69.
[47]Patel ZS,Mikos AG.Angiogenesis with biomaterial-based drug-and cell-delivery systems.J Biomater Sci Polym Ed 2004;15:701-26.
[48]Burdick JA,Vunjak-Novakovic G.Engineered microenvironments for controlled stem cell differentiation.Tissue Eng Part A 2009;15:205-19.
[49]Ribeiro-Filho LA,Sievert KD.Acellular matrix in urethral reconstruction.Adv Drug Deliv Rev 2015;82/83:38-46.
[50]Raya-Rivera A,Esquiliano DR,Yoo JJ,Lopez-Bayghen E,Soker S,Atala A.Tissue-engineered autologous urethras for patients who need reconstruction:an observational study.Lancet(London,England)2011;377:1175-82.
[51]Atala A.Engineering organs.Curr Opin Biotechnol 2009;20:575-92.
[52]Nuininga JE,Koens MJ,Tiemessen DM,Oosterwijk E,Daamen WF,Geutjes PJ,et al.Urethral reconstruction of critical defects in rabbits using molecularly defined tubular type I collagen biomatrices:key issues in growth factor addition.Tissue Eng Part A 2010;16:3319-28.
[53]Bullers SJ,Baker SC,Ingham E,Southgate J.The human tissue-biomaterial interface:arolefor PPARgammadependent glucocorticoid receptor activation in regulating the CD163+M2 macrophage phenotype.Tissue Eng Part A 2014;20:2390-401.
[54]Mauney JR,Nguyen T,Gillen K,Kirker-Head C,Gimble JM,Kaplan DL.Engineering adipose-like tissuein vitroandin vivoutilizing human bone marrow and adipose-derived mesenchymal stem cells with silk fibroin 3D scaffolds.Biomaterials 2007;28:5280-90.
[55]Korossis S,Bolland F,Southgate J,Ingham E,Fisher J.Regional biomechanical and histological characterisation of thepassiveporcineurinarybladder:implications for augmentation and tissue engineering strategies.Biomaterials 2009;30:266-75.
[56]Brown AL,Farhat W,Merguerian PA,Wilson GJ,Khoury AE,Woodhouse KA.22 week assessment of bladder acellular matrix as a bladder augmentation material in a porcine model.Biomaterials 2002;23:2179-90.
[57]Takahashi K,Yamanaka S.Induction of pluripotent stem cells from mouse embryonic and adult fibroblast cultures by defined factors.Cell 2006;126:663-76.
[58]Takahashi K,Tanabe K,Ohnuki M,Narita M,Ichisaka T,Tomoda K,et al.Induction of pluripotent stem cells from adult human fibroblasts by defined factors.Cell 2007;131:861-72.
[59]Takasato M,Er PX,Becroft M,Vanslambrouck JM,Stanley EG,Elefanty AG,et al.Directing human embryonic stem cell differentiation towards a renal lineage generates a selforganizing kidney.Nat Cell Biol 2014;16:118-26.
[60]Chen YT,Sun CK,Lin YC,Chang LT,Chen YL,Tsai TH,et al.Adipose-derived mesenchymal stem cell protects kidneys against ischemia-reperfusion injury through suppressing oxidative stress and inflammatory reaction.J Transl Med 2011;9:51.
[61]Cao H,Qian H,Xu W,Zhu W,Zhang X,Chen Y,et al.Mesenchymal stem cells derived from human umbilical cord ameliorate ischemia/reperfusion-induced acute renal failure in rats.Biotechnol Lett 2010;32:725-32.
[62]Togel F,Weiss K,Yang Y,Hu Z,Zhang P,Westenfelder C.Vasculotropic,paracrine actions ofinfused mesenchymal stem cells are important to the recovery from acute kidney injury.Am J Physiol Renal Physiol 2007;292:F1626-35.
[63]Yuan L,Wu MJ,Sun HY,Xiong J,Zhang Y,Liu CY,et al.VEGF-modified human embryonic mesenchymal stem cell implantation enhances protection against cisplatin-induced acute kidney injury.Am J Physiol Renal Physiol 2011;300:F207-18.
[64]Chen Y,Qian H,Zhu W,Zhang X,Yan Y,Ye S,et al.Hepatocyte growth factor modification promotes the amelioration effects of human umbilical cord mesenchymal stem cells on rat acute kidney injury.Stem Cells Dev 2011;20:103-13.
[65]Zhou Y,Xu H,Xu W,Wang B,Wu H,Tao Y,et al.Exosomes released by human umbilical cord mesenchymal stem cells protect against cisplatin-induced renal oxidative stress and apoptosisin vivoandin vitro.Stem Cell Res Ther 2013;4:34.
[66]Guan Y,Liu S,Liu Y,Sun C,Cheng G,Luan Y,et al.Porcine kidneys as a source of ECM scaffold for kidney regeneration.Mater Sci Eng C,Mater Biol Appl 2015;56:451-6.
[67]Yu YL,Shao YK,Ding YQ,Lin KZ,Chen B,Zhang HZ,et al.Decellularized kidney scaffold-mediated renal regeneration.Biomaterials 2014;35:6822-8.
[68]Guan Y,Liu S,Sun C,Cheng G,Kong F,Luan Y,et al.The effective bioengineering method ofimplantation decellularized renal extracellular matrix scaffolds.Oncotarget 2015;6:36126-38.
[69]Osman Y,Shokeir A,Gabr M,El-Tabey N,Mohsen T,El-Baz M.Canine ureteral replacement with long acellular matrix tube:is it clinically applicable?J Urol 2004;172:1151-4.
[70]Baltaci S,Ozer G,Ozer E,Soygur T,Besalti O,Anafarta K.Failure of ureteral replacement with Gore-Tex tube grafts.Urology 1998;51:400-3.
[71]Fu WJ,Xu YD,Wang ZX,Li G,Shi JG,Cui FZ,et al.New ureteral scaffold constructed with composite poly(L-lactic acid)-collagen and urothelial cells by new centrifugal seeding system.J Biomed Mater Res Part A 2012;100:1725-33.
[72]Xu Y,Fu W,Wang Z,Li G,Zhang X.A tissue-specific scaffold for tissue engineering-based ureteral reconstruction.PLoS One 2015;10:e0120244.
[73]Xu Y,Fu W,Li G,Shi J,Tan H,Hu K,et al.Autologous urothelial cells transplantation onto a prefabricated capsular stent for tissue engineered ureteral reconstruction.J Mater Sci Mater Med 2012;23:1119-28.
[74]Meng LC,Liao WB,Yang SX,Xiong YH,Song C,Liu LQ.Seeding homologous adipose-derived stem cells and bladder smooth muscle cells into bladder submucosa matrix for reconstructing the ureter in a rabbit model.Transplant Proc 2015;47:3002-11.
[75]Zhu WD,Xu YM,Feng C,Fu Q,Song LJ.Different bladder defects reconstructed with bladder acellular matrix grafts in a rabbit model.Der Urol Ausg A 2011;50:1420-5.
[76]Wang Y,Liao L.Histologic and functional outcomes of small intestine submucosa-regenerated bladder tissue.BMC Urol 2014;14:69.
[77]Zhao Y,He Y,Guo JH,Wu JS,Zhou Z,Zhang M,et al.Timedependentbladdertissueregenerationusingbilayer bladder acellular matrix graft-silk fibroin scaffolds in a rat bladder augmentation model.Acta Biomater 2015;23:91-102.
[78]Jiang X,Xiong Q,Xu G,Lin H,Fang X,Cui D,et al.VEGF-loaded nanoparticle-modified BAMAs enhance angiogenesis and inhibit graft shrinkage in tissue-engineered bladder.Ann Biomed Eng 2015;43:2577-86.
[79]Xiong Q,Lin H,Hua X,Liu L,Sun P,Zhao Z,et al.A nanomedicine approach to effectively inhibit contracture duringbladder acellular matrixallograft-inducedbladder regeneration by sustained delivery of vascular endothelial growth factor.Tissue Eng Part A 2015;21:45-52.
[80]Chen W,Shi C,Hou X,Zhang W,Li L.Bladder acellular matrix conjugated with basic fibroblast growth factor for bladder regeneration.Tissue Eng Part A 2014;20:2234-42.
[81]Chen W,Shi C,Yi S,Chen B,Zhang W,Fang Z,et al.Bladder regeneration by collagen scaffolds with collagen binding human basic fibroblast growth factor.J Urol 2010;183:2432-9.
[82]Zhou L,Yang B,Sun C,Qiu X,Sun Z,Chen Y,et al.Coadministrationof platelet-derivedgrowthfactor-BBand vascular endothelial growth factor with bladder acellular matrix enhances smooth muscle regeneration and vascularization for bladder augmentation in a rabbit model.Tissue Eng Part A 2013;19:264-76.
[83]Jiang X,Lin H,Jiang D,Xu G,Fang X,He L,et al.Co-delivery of VEGF and bFGF via a PLGA nanoparticle-modified BAM for effective contracture inhibition of regenerated bladder tissue in rabbits.Sci Rep 2016;6:20784.
[84]Zhou L,Xia J,Qiu X,Wang P,Jia R,Chen Y,et al.In vitroevaluation of endothelial progenitor cells from adipose tissue as potential angiogenic cell sources for bladder angiogenesis.PLoS One 2015;10:e0117644.
[85]Chen BS,Xie H,Zhang SL,Geng HQ,Zhou JM,Pan J,et al.Tissue engineering of bladder using vascular endothelial growth factor gene-modified endothelial progenitor cells.Int J Artif Organs 2011;34:1137-46.
[86]Zhang Y,Kropp BP,Lin HK,Cowan R,Cheng EY.Bladder regeneration with cell-seeded small intestinal submucosa.Tissue Eng 2004;10:181-7.
[87]Zhu WD,Xu YM,Feng C,Fu Q,Song LJ,Cui L.Bladder reconstructionwithadipose-derivedstemcell-seeded bladder acellular matrix grafts improve morphology composition.World J Urol 2010;28:493-8.
[88]Zhe Z,Jun D,Yang Z,Mingxi X,Ke Z,Ming Z,et al.Bladder acellular matrix grafts seeded with adipose-derived stem cells and incubated intraperitoneally promote the regeneration of bladder smooth muscle and nerve in a rat model of bladder augmentation.Stem Cells Dev 2016;25:405-14.
[89]Yuan H,Zhuang Y,Xiong J,Zhi W,Liu L,Wei Q,et al.Human umbilical mesenchymal stem cells-seeded bladder acellular matrix grafts for reconstruction of bladder defects in a canine model.PLoS One 2013;8:e80959.
[90]Yang SX,Yao Y,Hu YF,Song C,Wang LL,Jin HM.Reconstruction of rabbit urethra using urethral extracellular matrix.Chin Med J 2004;117:1786-90.
[91]Wang YQ,Li YQ,Liu LQ,Xu JJ,Huo R,Li Q,et al.[Rabbit urethral defect repair with freeze-dried acellular bladder submucosa].Zhonghua Zhengxing Waike Zazhi 2005;21:62-5[Article in Chinese].
[92]Huang X,Luo J,Liao Y,Qu Y,Yang Z.[Study on small intestinal submucosa as repair materials in urethral reconstruction].Zhongguo Xiufu Chongjian Waike Zazhi 2006;20:206-9[Article in Chinese].
[93]Lee M,Wu BM,Dunn JC.Effect of scaffold architecture and pore size on smooth muscle cell growth.J Biomed Mater Res Part A 2008;87:1010-6.
[94]Huang JW,Xie MK,Zhang Y,Wei GJ,Li X,Li HB,et al.Reconstruction of penile urethra with the 3-dimensional porous bladder acellular matrix in a rabbit model.Urology 2014;84:1499-505.
[95]Wang JH,Xu YM,Fu Q,Song LJ,Li C,Zhang Q,et al.Continued sustained release of VEGF by PLGA nanospheres modified BAMG stent for the anterior urethral reconstruction of rabbit.Asian Pac J Trop Med 2013;6:481-4.
[96]Lv X,Li Z,Chen S,Xie M,Huang J,Peng X,et al.Structural and functional evaluation of oxygenating keratin/silk fibroin scaffold and initial assessment of their potential for urethral tissue engineering.Biomaterials 2016;84:99-110.
[97]Jia W,Tang H,Wu J,Hou X,Chen B,Chen W,et al.Urethral tissue regeneration using collagen scaffold modified with collagen binding VEGfin a beagle model.Biomaterials 2015;69:45-55.
[98]Orabi H,Bouhout S,Morissette A,Rousseau A,Chabaud S,Bolduc S.Tissue engineering of urinary bladder and urethra:advancesfrom bench to patients.SciWorld J 2013;2013:154564.
[99]Fu Q,Deng CL,Song XF,Xu YM.Long-term study of male rabbit urethral mucosa reconstruction using epidermal cell.Asian J Androl 2008;10:719-22.
[100]Xie M,Song L,Wang J,Fan S,Zhang Y,Xu Y.Evaluation of stretched electrospun silk fibroin matrices seeded with urothelial cells for urethra reconstruction.J Surg Res 2013;184:774-81.
[101]Gu GL,Xia SJ,Zhang J,Liu GH,Yan L,Xu ZH,et al.Tubularized urethral replacement using tissue-engineered peritoneum-like tissue in a rabbit model.Urol Int 2012;89:358-64.
[102]Long JL,Zuk P,Berke GS,Chhetri DK.Epithelial differentiation of adipose-derived stem cells for laryngeal tissue engineering.Laryngoscope 2010;120:125-31.
[103]Koizumi NJ,Inatomi TJ,SotozonoCJ,FullwoodNJ,Quantock AJ,Kinoshita S.Growth factor mRNA and protein in preserved human amniotic membrane.Curr Eye Res 2000;20:173-7.
[104]Wang F,Liu T,Yang L,Zhang G,Liu H,Yi X,et al.Urethral reconstructionwithtissue-engineeredhumanamniotic scaffold in rabbit urethral injury models.Med Sci Monit Int Med J Exp Clin Res 2014;20:2430-8.
[105]Li CL,Liao WB,Yang SX,Song C,Li YW,Xiong YH,et al.Urethral reconstruction using bone marrow mesenchymal stem cell-and smooth muscle cell-seeded bladder acellular matrix.Transplant Proc 2013;45:3402-7.
[106]Li C,Xu YM,Liu ZS,Li HB.Urethral reconstruction with tissue engineering and RNA interference techniques in rabbits.Urology 2013;81:1075-80.
[107]Zhang K,Guo X,Zhao W,Niu G,Mo X,Fu Q.Application of Wnt pathway inhibitor delivering scaffold for inhibiting fibrosis in urethra strictures:in vitroandin vivostudy.Int J Mol Sci 2015;16:27659-76.
[108]Huang JW,Lv XG,Li Z,Song LJ,Feng C,Xie MK,et al.Urethral reconstruction with a 3D porous bacterial cellulose scaffold seeded with lingual keratinocytes in a rabbit model.Biomed Mater(Bristol,England)2015;10:055005.
[109]Atala A,Danilevskiy M,Lyundup A,Glybochko P,Butnaru D,Vinarov A,et al.The potential role of tissue-engineered urethral substitution:clinical and preclinical studies.J Tissue Eng Regen Med 2015;11:3-19.
[110]Dvorin EL,Wylie-Sears J,Kaushal S,Martin DP,Bischoff J.Quantitative evaluation of endothelial progenitors and cardiac valve endothelial cells:proliferation and differentiation on poly-glycolic acid/poly-4-hydroxybutyrate scaffold in response to vascular endothelial growth factor and transforming growth factor beta1.Tissue Eng 2003;9:487-93.
[111]Cattan V,Bernard G,Rousseau A,Bouhout S,Chabaud S,Auger FA,et al.Mechanical stimuli-induced urothelial differentiation in a human tissue-engineered tubular genitourinary graft.Eur Urol 2011;60:1291-8.
[112]Duan B,Hockaday LA,Kang KH,Butcher JT.3D bioprinting of heterogeneous aortic valve conduits with alginate/gelatin hydrogels.J Biomed Mater Res Part A 2013;101:1255-64.
[113]Phillippi JA,Miller E,Weiss L,Huard J,Waggoner A,Campbell P.Microenvironments engineered by inkjet bioprinting spatially direct adult stem cells toward muscle-and bone-like subpopulations.Stem Cells(Dayton,Ohio)2008;26:127-34.
 Asian Journal of Urology2018年2期
Asian Journal of Urology2018年2期
- Asian Journal of Urology的其它文章
- Overcoming scarring in the urethra:Challenges for tissue engineering
- Emergency treatment of male blunt urethral trauma in China:Outcome of differentmethods in comparison with other countries
- Prevention strategies for ureteral stricture following ureteroscopic lithotripsy
- Management of complex and redo cases of pelvic fracture urethral injuries
- The association of benign prostatic hyperplasia with lower urinary tract stones in adult men:A retrospective multicenter study
- The effect of adjunct caudal block on postoperative analgesia in robot-assisted laparoscopic radical prostatectomy:A prospective randomized controlled,single blinded pilot study in a tertiary centre