
Adaptive Radiotherapy for Lung Cancer
2019-04-15 08:16HualiangZhongAllenLi
腫瘤預防與治療 2019年1期
Hualiang Zhong, X. Allen Li
Department of Radiation Oncology, Medical College of Wisconsin, Milwaukee, Wisconsin, USA
[Abstract] The concept of adaptive radiotherapy (ART) was proposed 20 years ago, and since then a variety of methodologies and techniques have been developed to accommodate different clinical requirements, including both online and offline plan adaptations. Compared with pre-treatment planning, plan adaptation involves more computational tasks and consequently has increased complexity and computational burden. While ART can benefit many cancer patients, challenges still exist in development and implementation of high-quality ART programs. In this short review, we will focus on the development of offline ART for lung cancer. We will also discuss the advantages and disadvantages of different clinical implementations of ART.
[Key words] Adaptive radiotherapy; Lung cancer; Plan adaptation
INTRODUCTION
Adaptive Radiation Therapy (ART) is a state-of-the-art approach that uses a treatment feedback process to account for patient-specific anatomic and/or biological changes, thus, delivering highly individualized radiation therapy for cancer patients[1]. ART strategies include offline and online adaptations. Offline ART generates a new radiation treatment (RT) plan based on the images acquired during the RT delivery session, accounting for information from previous treatment fractions, and delivers the new plan for subsequent fractions to correct for systematic variations[2]. In contrast, online ART generates a new plan based on the image of the day and delivers the new plan for that day’s fraction accounting for both random and systematic changes[3-4]. This work will review technical aspects of offline ART based on its applications for lung cancer.
It has been well documented that advanced RT technologies have significantly improved radiation treatment outcome for lung cancer. For example, a large population-based study showed that IMRT improves overall survival for patients with T3 and T4 tumors[5]. Another example is on-board imaging (OBI) which helps reduce patient setup errors and minimize radiation toxicity to surrounding normal tissue. With the assistance of OBI, stereotactic body radiotherapy (SBRT) has significantly improved clinical outcomes[6-9]. The emergence of MRI-Linac may further enhance the capabilities of real-time tracking for intra-fractional tumor motion, and online plan adaptation could consequently be achieved by making radiation beams conformal to tumor targets throughout the whole treatment course[4,10-11].
Different from lung SBRT which has been reported to be an efficient treatment modality, dose escalation for locally advanced cancer patients has not yet been implemented in clinic because escalating target dose may result in the increased risk of normal tissue complications[12-14]. On the other hand, tumor volumes may change during the course of treatment. For example, with 1.2% daily tumor regression as reported in literature, the pre-treatment plan can be adapted with beams conformal to reduced tumor targets. This may help increase target dose, reduce normal tissue toxicity, and thereby improve treatment outcomes for these patients[15-17]. These pre-clinical studies have highlighted the importance of clinical implementation of adaptive radiotherapy. Since ART involves many techniques and can be applied to different clinical scenarios, it is not feasible to introduce all the aspects of this treatment modality in a short review. Instead, this article will go through the major technical components developed for off-line plan adaption for patients with locally advanced lung cancer.
TECHNICAL DEVELOPMENT
ART involves many tasks such as developing an initial treatment plan, evaluating treatment response using computed tomography (CT), cone beam computed tomography (CBCT) or positron emission tomography (PET) images, and making decisions on plan adaptation. If required, an adaptive plan will be developed that includes re-contouring, dose accumulation, plan re-optimization, and quality assurance. In the following sections we will discuss the current status of technical development for each of these tasks.
Contour re-generation
Contour delineation for tumor targets and organs at risk is a time-consuming process in treatment planning[18]. While frequent plan adaptations may help maximize the benefits of ART[19], transitional gains in each adaptation step may be counteracted by tremendous efforts put in re-contouring and other re-planning tasks. To address this issue, different approaches were developed to automatically generate contours. Various 2D or 3D auto-segmentation techniques such as region-growing and “snake” algorithms have been developed for direct segmentation of different anatomic structures such as bone, pancreas, heart, esophagus[20-21]; deformable image registration (DIR) algorithms have also been employed to automatically propagate contours from the original planning CT images to during-RT images[22-23]. Due to limited contrasts and gradients in during-RT images, the registrations could have large errors, and the propagated volumes need to be thoroughly assessed[9].
Atlas-based segmentation methods are expected to segment image structures that have no obvious intensity differences, where theaprioriinformation about the difference between these objects can be incorporated in spatial relationship or statistical models[24]. Recent developments in machine learning have revolutionized the field of artificial intelligence. Deep learning algorithms, especially deep convolutional neural networks (DCNN), are a powerful methodology for solving challenging medical imaging problems such as tumor detection, disease classification, and structure segmentation[25]. Different atlas-based segmentation approaches could consequently be enhanced by the developed machine learning techniques[26].
Deformable image registration (DIR)
Deformable registration of two images is to establish a correspondence map that matches anatomical structures in one image to their counterparts in the other image. The counterparts could be the same structures appeared in the two images acquired at different times or with different modalities. In adaptive radiotherapy, longitudinal images are often acquired at different treatment stages for treatment planning, patient setup, tumor localization, or treatment response assessment. To use these images correctly, the acquired images need to be registered to a reference image such that information contained in these images can be appropriately interpreted or assessed. DIR is a key component in development of adaptive radiotherapy techniques and is required almost at every step in the process of plan adaptation. Except the contour propagation mentioned before, dose accumulation, 4D planning and treatment response assessment all require accurate DIR. Development of an appropriate DIR algorithm for each of these subjects is an active area of research.
Over the last two decades many registration algorithms have been developed, among which the optical flow-based “demons” and B-spline-based free form are two major algorithms developed in many free and commercial software packages[27-28]. These algorithms have been modified or improved over the years for different applications. For example, Yang et al generated inverse consistent DVFs to improve the accuracy of the demons registration[29]and Vercauteren et al made the underlying transformation diffeomorphic to generate more smooth deformation fields[30-31]; Rueckert et al made the parametric B-spline-based registration algorithm diffeomorphic[32], which was then extended to be hierarchical[33]and to have non-uniform knot placements[34]and simplified regularizations[35]. The B-Spline and demons algorithms could be combined with a mechanical model-based finite element method (FEM) to register anatomical structures in the case of large-scale deformation[36-37]. These methods were extended to registration of soft tissue in low contrast regions[38]and between different modality images[39]. The mechanical model-based hybrid registrations could also reduce registration errors in the neighborhood of regressing tumors (Figure 1), and meanwhile maintain the integrity of dose mapping[39-40]. These technical developments have enhanced the efficiency of structure contouring and dose accumulation and improved the quality of adaptive radiotherapy[9, 41-42].
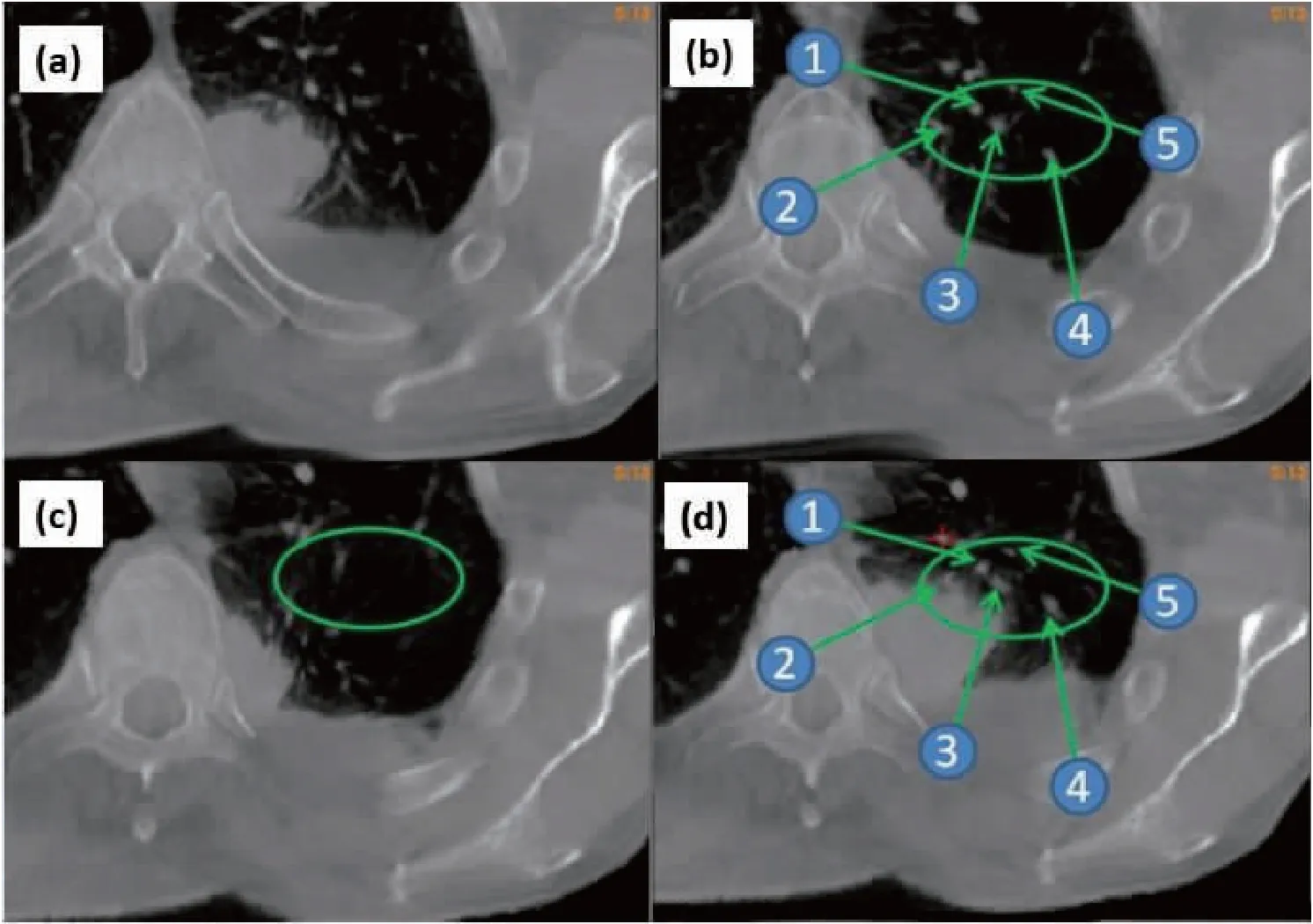
Figure1.CBCTImages
CBCT images acquired at fraction 1 and 25 shown in (a) and (b), respectively; (c) the warped source image (fraction 1) using VelocityAI, and (d) the warped source image using the FEM-based hybrid method, resulting in landmarks consistent to their positions at fraction 25.
It should be mentioned that computational time for DIR currently is not yet sufficient for online ART. The computation speed may depend on multiple factors such as image size, parametric resolution and number of iterations implemented in these algorithms, and simplifying these parameters may compromise the accuracy of deformable registration[43]. To address these issues, Gu et al demonstrated that the GPU-enhanced demons algorithm could complete 4D-CT image registrations around 10 seconds[44]. In contrast, while B-spline-based registration algorithms are capable of performing both unimodal and multimodal registrations, it is difficult to improve the speed of these algorithms due to their computational complexity.
Accumulation of delivered doses
To develop an adaptive plan for the remaining treatment fractions, radiation dose delivered up-to-date needs to be accumulated in each image voxel. The accuracy of dose accumulation depends on dose mapping and its underlying DIR methods used. Most registration algorithms could currently be accurate within 2~3 mm on average[43, 45-46]which is comparable to the resolution of dose grids often used in clinic[47-48], while some algorithms could have the mean error up to 6.9 mm[46]. The registration errors may induce dose mapping uncertainties up to 3 Gy/mm[49], and the clinical impact of the spatial errors may need further investigations[50].
With a correct registration map, dose delivered at each fraction could be mapped to a reference image and summated to get the total dose. However, dose interpolation methods may induce dose mapping errors in regions with high dose gradients, and some large errors even not at a steep dose gradient[51]. The latter could be due to different formations of image grids between the source and target images. Deformable dose accumulation (DDA) could also be compromised by changes in the mass and volume of solid tumors and/or normal tissue over the course of treatment. To address these issues, 4D Monte Carlo-based methods such as voxel-warping method (VWM)[52], energy-mass congruent mapping (EMCM)[53]and energy-conserved registration methods[39, 54]were proposed to help improve the quality of dose accumulation. Recently EMCM was applied to model-based dose calculation algorithms in a commercial software package[39-40], and its computation speed was improved significantly by using a GPU-based computational approach[55].
Quality assurance
Adaptive treatment planning involves 3D dose calculation, DIR, contour propagation, dose warping and accumulation. Ideally each of these tasks could be evaluated separately for each patient. Different from conventional dose calculation algorithms which can be verified with homogeneous and heterogeneous dosimetric phantoms, the total dose delivered to deforming organs over the course of treatment is difficult to verify. This is mainly due to the lack of a gold standard required to evaluate the DIR and DDA operations[56]. It is necessary to have independent verifications of dose accumulation for each patient. In general, two kinds of verifications can be performed.
Spatial accuracy: landmark and contour consistencies and DICE similarity coefficients are often used as criteria to evaluate the performance of DIR in different applications[46, 57-59], and the self and inverse consistencies of deformation maps have also been used to evaluate the accuracy of the registration[29, 60-61]; computational phantoms offer another option to verify the accuracy of displacements at all voxels in the registered images. The phantom’s deformation can be simulated using different mathematical formulae[62]. With the aid of the finite element method, Stanley et al created a patient-specific deformable model to improve the realism of tissue deformation for a lung cancer patient[63]. The FEM-computed deformable model and a deformable dosimetry were overlaid as shown in Figure 2 (a).

Figure2.TheFEM-computedDeformableModelandaDeformableDosimetry
(a) A lung patient CT image overlaid on its warped image using a patient-specific FEM model; (b) a deformable dosimetry phantom; (c) the CT image of the dosimetry phantom.
Dosimetry accuracy: different from computational phantoms, physical phantoms may help measure the delivered dose to verify dose accumulation operations. Figure 2 (b) showed a deformable phantom containing heterogeneous sponges for simulating respiratory motion. The phantom with deformation automatically driven by a motor was irradiated, and delivered doses were measured by imbedded thermoluminescent dosimeters (TLDs). However, these phantoms are unable to simulate mass changes in tumors and other organs while these changes are often observed during the course of treatment. Also these phantoms do not show realistic organ deformation and mass heterogeneity as patients, so further improvement of these phantoms is highly desired[64-66]. It was suggested that the phantom-based evaluations should be supplemented by other verification methods such as the energy conservation criterion that can be applied to both deformed anatomical structures and regressed tumor volumes[39, 54].
CLINICAL IMPLEMENTATION
When patients have large spatial changes in tumor targets or organs at risk, it is important to have the initial treatment plan adapted. Different adaptive planning strategies, however, could result in different clinical outcomes.
Applications of adaptive radiotherapy
As the PTV is generally large for locally advanced non-small-cell lung carcinoma (NSCLC), the initial treatment plan often show high radiation dose to healthy tissue. For example, the treatment regimen of 30×2 Gy to tumor targets may cause mean lung dose (MLD) to exceed 20 Gy for patients with bulky tumors. On the other hand, it was observed that lung tumors regress of about 50% volume over the course of fractionated RT[16-17, 67-69]. For these patients, radiation beams could be reshaped to the residual tumor target after delivering a number of treatment fractions, and this may reduce radiation toxicity to surrounding tissue.
Radiation therapy with the radiation target field updated during the course of treatment has recognized potential to benefit patients (the NRG/RTOG Trial No. 1106)[70-72]. It was reported that escalating radiation dose may help improve tumor locoregional control and overall survival[73-74]. With tumor regression, high-quality ART may ensure iso-toxic dose escalation which may consequently help improve clinical outcomes[75-77].
In addition, radiation treatment may change anatomical structures and physiological functions. For example, airway obstruction could be alleviated after a few weeks of treatment. This will allow the collapsed lung structures re-ventilated. Respiratory patterns could consequently change and the relative positions of lung and other structures could be different after the treatment. The atelectatic changes combined with anatomical variations may render it necessary to update the pretreatment plan for the remaining treatment fractions[68].
Frequency of plan adaptation
As tumor continuously shrinks during the course of treatment, there is a trade-off between the amount of the reduced tumor volume and the number of the remaining fractions[69]. It has been reported that plan adaptation performed around fraction 15 and fraction 20 is most dosimetrically efficient for concurrent and sequential chemo-radiotherapy, respectively. Based on iso-toxic mean lung dose (MLD), re-planning twice at weeks 2 and 4 may achieve an average escalation of 13.4 Gy[71], and at weeks 3 and 5 may have an average increase of 7 Gy on tumor targets. Since tumor shrinkage depends on many factors such as tumor histology, location, stage and imaging modality used in the volume measurement, the optimal time point for plan adaptation and its dosimetric gain could have variations for individual patients.
The benefits of adaptive planning in terms of normal tissue sparing have also been investigated by multiple investigators. Guckenberger et al showed that when the GTV volume reduced 39% on average, a single plan adaptation at the end of week 4 was able to reduce MLD by 100 cGy on average[19, 77]. Dial et al demonstrated that the mid-treatment plan adaptation reduced MLD by 38 cGy for patients having an average GTV reduction of 21% at the end of the treatment[19]; Woodford et al found that the MLD reductions are in the range of 30 to 160 cGy for three patients[78]. These results suggested that the majority of the gains from ART can be achieved by implementing a single mid-treatment adaptation if the tumor volume regresses by 30% within the first 20 fractions[78].
It should be mentioned that large uncertainties may exist in the measurement of residual tumor volumes. For example, internal hemorrhage, necrosis, or metabolically non-viable tumor cells could be mis-counted in the measured volume, especially when only CBCT images were used for the volume measurement[17]. Compared to CT or CBCT images, FDG-PET images can show metabolic activities in addition to the tumor volume. It was therefore recommended that both CT and PET images shall be used for the mid-treatment tumor response measurement for adaptive RT[70,79]. Note that the standardized uptake value (SUV) of PET images could be influenced by many factors[80-82], and changes in region-specific SUVs cannot be quantified until the correspondent images are correctly registered[82-84]. While the Response Evaluation Criteria in Solid Tumors (RECIST) has been used as a criterion for evaluation of tumor response in clinic[85], methods for quantitative assessments of tumor response, in addition to tumor volume measurements, are worth further investigations.
Dose regimens for adaptive planning
It has been reported that for locally advanced NSCLC, dose regimens in the range of 60~66 Gy have 5-year overall survival rates at 10%~15%[86]. Although a randomized trial did not show superiority at a dose of 74 Gy[14], the reasons for the underperformance of the higher dose arm are still unclear[87-89]. Technical factors such as respiratory motion management, treatment planning margin, delivery mode (IMRTvs3D-CRT) and imaging modality used for treatment planning and delivery all could have impacts on the clinical outcomes, and each of these components may be worth further investigations[87,90]. It was reported that for patients with locally advanced NSCLC, adaptive planning increases radiation dose up to 80 Gy on average on the residual tumor without increasing MLD[68,71]. In general, improved treatment planning and delivery techniques will help better spare lung, heart and other healthy organs from irradiation[86].
For lung cancer patients, it has been reported that increasing dose from 60 Gy to 74 Gy results in predictable, deleterious effects on quality of life[91]. For these patients, RT-induced adverse events may include pneumonitis, esophagitis and pericarditis[92], and therefore radiation dose to these organs should be minimized. Compared to dose escalation, it is of equivalent importance to develop effective treatment strategies to mitigate normal tissue toxic effects for these patients. It was shown that for iso-prescription adaptive plans (relative to initial plans), mean lung dose was reduced, on average from 17.3 Gy (initial plan) to 14.8 Gy for the adapted plans[68,71]. It is worth conducting clinical trials to compare clinical gains of different ART strategies, e.g.: iso-toxic dose escalationvsiso-prescription, for plan adaptation. It has been reported, recently, from a phase 2 clinical trial that PET-CT guided ART for locally advanced NSCLC improved local-regional control[93]. With more clinical data being collected on locoregional control and overall survival, it will be possible to develop optimized dose regimens and treatment protocols for ART.
DISCUSSION
Since patients with locally advanced NSCLC often have tumor regression during the course of fractionated radiotherapy, updating their initial RT plan may help enable dose escalation to residual tumor targets and spare normal tissue. Pre-clinical studies have shown a great promise for adaptive radiotherapy to treat these patients. Different strategies such as iso-toxic target dose escalation or iso-prescription normal tissue sparing have been proposed for plan adaptation. The emergency of onboard imaging, especially MRI-Linac, has rendered ART an imperative treatment modality for many patients. While significant progress has been made in the past twenty years for automatic contouring, image registration, dose accumulation and re-planning algorithms, ART techniques remain to be improved before they can be routinely used for treatment of NSCLC patients[94].
Since DIR plays multiple roles in ART, registration accuracy is still the major concern for the clinical implementation of ART. It has been illustrated that intensity-based DIR algorithms are prone to have errors in regions with low image contrasts[43,45,95], and tumor regression may also cause registration errors in nearby normal tissue. For every 10% regression in tumor volume, the dose error associated with a rigid (non-deformable) registration algorithm for computing accumulated dose is approximately 1 Gy[68]. The large dose errors (up to 5~6 Gy for 50% tumor regression) will downgrade the quality of adaptive therapy and are likely to impact treatment outcomes[56]. Due to the lack of knowledge on the pattern of tumor regression, how to deform the anatomical structures nearby the tumor is still unclear[68,72]. While mechanical models have been introduced to improve registration accuracy, their parameters and constraints still need to be optimized. Since registration errors could be propagated to dose reconstruction and response assessment, the accuracy of these algorithms in clinical settings needs to be further evaluated. Also with DIR used in more clinical applications, computational speeds for FEM or B-Spline-based registrations need to be improved.
Different from development of an initial treatment plan, CTV margins required for an adaptive plan could depend on the precision and efficiency of delivered treatment. Since tumor response is not uniform, survived tumor cells may exist sporadically. Similar to sub-clinical disease spread from initial gross tumor volumes, tumor cells may survive in the regions surrounding the residual tumor, and these regions still need to be covered by an updated CTV for the adaptive plan[96]. While PET images, after appropriate registrations, may help identify regions with high metabolic activities, the resolution of these images is limited, and the survived tumor cells cannot be detected effectively. Since treatment efficacy is patient dependent, it is not straightforward to find the optimal dose required to eliminate the remaining tumor cells.
Adaptive planning strategies, with different dose levels assigned to the remaining tumor and to the regions with subclinical diseases, respectively, have been considered in clinical trials[90]. Different from the sub-volume boosting to each segment in these trials, dose painting has also been proposed by using a voxel-level dose prescription based on image intensity changes in individual pixels[97]. The quantitative use of images, termed as theragnostic imaging, may help determine the minimal radiation dose required to treat individual patients. When image quantities are directly associated with radiation dose, the quality of these images and their derivatives should be reviewed with high standard criteria.
Pre-clinical studies have shown that ART may help optimize treatment regimens, improve clinical outcomes, and consequently benefit many cancer patients. It is worth improving adaptive planning techniques and meanwhile investigating the efficacy of different ART strategies with more clinical trials.
